

When a baby only sleeps when held, it usually means their nervous system feels safest and most regulated against a parent’s body. The warmth, heartbeat, and motion mimic the womb and help an immature system shift from alert to calm. For most newborns, this is normal and expected. But when it persists alongside other signs of stress, it can point to a nervous system stuck in high alert and struggling to settle on its own.
If you’re reading this while pinned to the couch by a sleeping baby, afraid to move an inch, you are not alone. This is one of the most common and most exhausting challenges new parents face. You’ve probably been told it’s “just a phase” or a “bad habit.” Sometimes that might be true. But sometimes there’s a deeper reason your little one can’t downshift into rest unless they’re in your arms, and almost no one is talking about it.
Here’s what makes this different from the standard sleep advice you’ll find everywhere else: we’re going to look at why the body behaves this way at the level of the nervous system — and what it means when contact sleep is less about preference and more about a baby who can’t find their own “off switch.” You’ll learn the normal reasons babies sleep better when held, the signs that something more is going on, and where root-cause, Neurologically-Focused Chiropractic Care fits in.
Why Does My Baby Only Sleep When Held?
A baby sleeps better when held because being against a parent’s body recreates the conditions of the womb—warmth, the sound of a heartbeat, gentle motion, and steady pressure—which signal safety to an immature nervous system and help it shift into rest. Newborns can’t yet regulate their own temperature, arousal, or stress response well, so they borrow yours. Being held literally helps steady their breathing, heart rate, and stress chemistry.
This is rooted in real biology. Research on infant physiology shows that being carried produces an automatic calming response, heart rate slows, and crying and voluntary movement decrease. A coordinated reaction that appears to be hardwired to support being transported by a caregiver. In other words, your baby isn’t being manipulative or spoiled. They’re following instinct.
There are a handful of normal, expected reasons this happens in the early months:
- The fourth trimester. For the first three to four months, babies are still adjusting to life outside the womb. Closeness isn’t a luxury; it’s how they co-regulate.
- The Moro (startle) reflex. This primitive reflex makes babies fling their arms out and jerk awake when they sense a change in position, like being lowered into a crib. It typically fades by four to six months.
- Immature sleep cycles. Newborns move through light sleep often and wake easily between cycles, looking for the same conditions they fell asleep in.
- Sleep associations. As babies get older, they can come to depend on being held, rocked, or fed to fall asleep, so they need that same input to fall back asleep.
For many families, this resolves as the baby matures. But for some, the pattern is stubborn, intense, and paired with other signs of a stressed system, and that’s where the conversation needs to go deeper than swaddles and white noise.
What Does It Mean When a Baby Can’t Sleep Unless Held?
When a baby genuinely cannot settle unless held—fighting sleep, startling constantly, sleeping only 20 to 30 minutes at a time, never seeming truly rested—it can be a sign that their Autonomic Nervous System is stuck in a state of high activation and can’t shift into deep, restorative sleep on its own. The body knows how to fall asleep; what it struggles with is the neurological gear-shift into calm.
To understand this, picture the Autonomic Nervous System using the gas pedal and brake pedal analogy. The Sympathetic Nervous System is the “gas pedal,” fight or flight, alertness, activation. The Parasympathetic Nervous System is the “brake pedal,” rest, digest, and regulate. A well-regulated baby can ease off the gas and press the brake to drift into sleep. A dysregulated baby has a stuck gas pedal: they’re wired and exhausted at the same time, what we often describe as wound up and worn out.
This is where the vagus nerve comes in. The vagus nerve is the longest cranial nerve in the body, carrying parasympathetic “rest and digest” signals between the brain and major organs, including the heart, lungs, and digestive system. Vagal tone, a measurable indicator of how well that nerve is working, is closely tied to a child’s ability to calm, digest, and sleep. When vagal tone is low, the brake pedal is weak, and the baby can’t access deep rest without an outside source of regulation: you. Your heartbeat, breathing, and warmth act as a borrowed brake pedal. The baby isn’t choosing dependence; their own system can’t yet do the job on its own.
How This Connects To Other Childhood Conditions
Babies who can’t self-regulate into sleep frequently share an underlying thread with children later diagnosed with Autism, ADHD, and Sensory Processing Disorder. This co-occurrence isn’t a coincidence. All of these conditions share a common root in pediatric dysautonomia, a dysfunction of the Autonomic Nervous System that keeps a child stuck in sympathetic dominance, unable to fully access the calm, regulated states needed for sleep, digestion, and emotional control. Persistent sleep struggles in infancy can be one of the earliest visible signs that a nervous system is working harder than it should to regulate itself.
What Causes a Baby’s Nervous System to Get Stuck in High Alert?
A baby’s nervous system can get locked in high alert through a sequence of early stressors that build on one another. What we call the “Perfect Storm,” is a framework developed by Dr. Tony Ebel. It describes how prenatal stress, birth trauma, and early childhood stressors stack up and shift a developing nervous system toward sympathetic dominance, leaving it unable to downshift into rest, digestion, and regulation.
The sequence usually unfolds like this:
- Prenatal stress: High maternal stress during pregnancy sends stress hormones like cortisol across the placenta, which can shape a more reactive nervous system before birth. A 2017 study in Development and Psychopathology found that infants exposed to more stressful life events during gestation showed greater autonomic reactivity and weaker recovery, measured through their Parasympathetic Nervous System physiology.
- Birth trauma: Interventions like C-section, forceps, vacuum extraction, induction, or prolonged labor can place physical strain on a baby’s upper neck and brainstem, exactly where the vagus nerve exits the skull. Even “textbook” vaginal deliveries involve significant pressure and twisting forces on the head and neck.
- Early childhood stressors: Reflux, colic, frequent ear infections, antibiotics, environmental toxins, and other early strains keep adding load to an already-taxed system.
When these stack up, the body can settle into a protective fight-or-flight pattern that was meant to be temporary but instead becomes the baseline. The gas pedal stays pressed. And one of the very first places parents notice it is sleep, because true rest requires the parasympathetic brake to take over. Dr. Ebel describes sleep as the body’s reset button. A baby stuck in sympathetic dominance may doze briefly but never fully drops into deep, restorative sleep. They’re tired but can’t rest, so they reach for the one reliable source of calm they know: being held.
What Is a Subluxation and How Does It Affect a Baby’s Sleep?
Subluxation is stress to the neurospinal system, which includes three components: physical misalignment, joint fixation (loss of normal motion), and neurological interference (disrupted nerve signaling between the brain and body). In babies, the upper neck and brainstem are the most vulnerable areas—and not coincidentally, this is where birth forces concentrate and where the vagus nerve and key sleep-regulating pathways travel.
When subluxation creates interference in this region, it can keep the nervous system tilted toward the sympathetic side and dampen the parasympathetic, vagal “brake.” That’s a direct hit to the systems a baby relies on to calm down and stay asleep. The result is often a baby who’s hard to settle, startles easily, wakes the instant they’re put down, and seems to need constant input to stay regulated.
There’s clinical research that lines up with this picture. A 2021 study in Frontiers in Pediatrics evaluated 120 colicky babies and found that nearly all of them showed measurable signs of vestibular and brainstem dysregulation, including heightened startle (Moro) responses, compared to non-colicky infants, and that gentle manual care was associated with improvements in these markers. The same brainstem regulation that governs the startle reflex and calming responses is deeply tied to whether a baby can settle into sleep.
This is why simply “fixing the habit” with sleep training sometimes doesn’t work for these babies. If the underlying issue is a nervous system that can’t access its brake pedal, no amount of routine alone resolves it. You have to address the regulation problem at its source.
How Can You Tell Normal Contact Sleep From a Nervous System Issue?
Normal contact sleep looks like a baby who settles fairly easily when held, sleeps peacefully, transfers to a flat surface at least some of the time, and is generally content when awake. A nervous-system-driven pattern looks different: the baby fights sleep hard, startles or arches constantly, sleeps only in very short stretches, wakes the second they’re set down, and often struggles in other areas too.
Signs that point toward deeper nervous system dysregulation rather than a simple phase include:
- Sleeping only 20–30 minutes at a time and never seeming truly rested
- A high-pitched, hard-to-console cry
- Frequent back-arching, stiffening, or a body that feels tense
- Difficulty latching, feeding challenges, or a strong preference to turn one direction
- Reflux, colic, excessive spit-up, gas, or constipation
- Startling violently at small sounds or movements
- Seeming “wired,” alert, and unable to wind down even when clearly exhausted
When sleep struggles accompany several of these, it’s worth looking beyond sleep-training tactics and considering how well the baby’s nervous system is regulating overall. These patterns cluster because they share the same root: an autonomic system stuck in overdrive. And none of it means you’ve done something wrong; a dysregulated nervous system is a physiological problem, not a parenting failure.
How Does Neurologically-Focused Chiropractic Care Help Babies Sleep?
Neurologically-Focused Chiropractic Care is a specialized form of pediatric chiropractic that identifies and corrects subluxation patterns affecting the Autonomic Nervous System, using neurological assessment and gentle, child-specific adjustments to restore regulation. For a baby who only sleeps when held, the goal isn’t to force independent sleep; it’s to help the nervous system find its own brake pedal so rest becomes possible.
The starting point is assessment, not adjustment. PX Docs offices use INSiGHT Scans, a three-part neurological assessment:
- Heart rate variability (HRV) measures autonomic balance
- Surface electromyography (sEMG) measures muscle tension patterns
- Thermal scanning measures Autonomic Nervous System function.
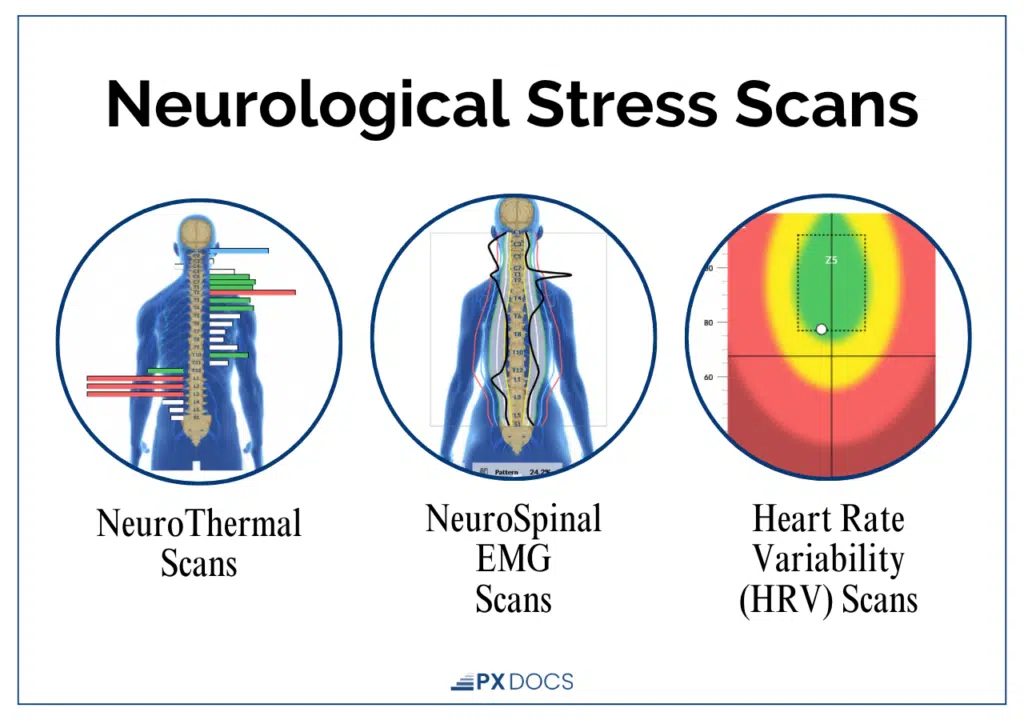
These scans show whether a baby is stuck in sympathetic dominance and where tension and interference are concentrated, giving parents an objective picture instead of guesswork. Importantly, INSiGHT scans are not a treatment or a cure for any condition, not even back pain. They’re a measurement tool.
From there, care focuses on gentle adjustments, about the pressure you’d use to check a tomato for ripeness, to reduce interference in the upper neck and brainstem region and support better vagus nerve function and vagal tone. As the parasympathetic “brake” comes back online, many families report their child begins to settle more easily, sleep longer stretches, and rely less on constant holding.
Take Rhodes, for example. His active startle reflex kept waking him throughout the night. With consistent Neurologically-Focused Chiropractic Care, his nervous system became more regulated, and now he’s sleeping through the night.
What makes this approach different from conventional sleep advice is the order of operations. Instead of starting with the behavior (the contact napping) and trying to train it away, NFCC starts with the physiology (the dysregulated nervous system). When the root cause is addressed, the behavior often shifts on its own because the baby finally can do what we were asking of them.
What Can Parents Do At Home To Help a Baby Who Only Sleeps When Held?
Parents can support a held-only sleeper at home by gently recreating the regulating input of being held while slowly building the baby’s capacity to settle on their own. The aim isn’t to abruptly take away comfort. What we’re trying to do is to help an immature or overstressed nervous system practice downshifting with support. These strategies work alongside, not instead of, addressing any underlying regulation issue:
- Warm the sleep surface first. A cold sheet can trigger the startle reflex. Briefly warm the bassinet (then remove the heat source) to make the transfer feel less jarring.
- Transfer feet-first, fully drowsy. Lower the bottom and legs before the head to reduce the sensation of falling that fires the Moro reflex.
- Use steady white or pink noise. It echoes the constant sound babies hear in the womb and masks startling household noises.
- Swaddle (until rolling). A snug swaddle recreates womb pressure and limits the startle reflex. Stop once your baby shows signs of rolling.
- Try “drowsy but awake.” Lay your baby down, sleepy but not fully out, so they practice settling in their own space.
- Start with one nap a day. Pick the calmest nap to practice crib sleep and keep the others as contact naps for now.
If you’ve worked these strategies consistently and your baby still can’t settle without being held, especially alongside the stress signs above, that’s your cue to look deeper rather than push harder. Persistent dysregulation needs support at the nervous system level.
The Bottom Line
When your baby only sleeps when held, it’s usually their nervous system telling you it feels safest and most regulated in your arms, and in the early months, that’s perfectly normal. The warmth, heartbeat, and motion of being held act as a borrowed brake pedal for a system that can’t yet slow itself down. For most babies, this softens with time.
But when contact sleep is intense, stubborn, and traveling with signs of stress, constant startling, very short sleep, feeding or digestive struggles, it can be an early signal that the Autonomic Nervous System is stuck in high alert and can’t access deep rest on its own. That’s a physiology problem, not a parenting failure, and it can be supported. When gentle strategies aren’t enough, a root-cause neurological assessment can reveal what’s really going on.
Trust your instincts. If something feels off beyond the usual newborn fog, it’s worth a closer look. To find a trained pediatric provider near you, visit the PX Docs Directory and connect with a doctor who can assess your baby’s nervous system and help them—and you—finally get some rest.
Frequently Asked Questions
Is it normal for my newborn to only sleep when held?
Yes. In the first three to four months, it’s completely normal for a newborn to sleep best when held. Their nervous system is still immature and relies on the warmth, heartbeat, and motion of a caregiver to feel safe and shift into rest. Contact sleep during this stage is developmentally expected and not a bad habit. It’s worth a closer look when it’s intense, persistent, and paired with other signs of stress, like constant startling, very short sleep, or feeding and digestive troubles.
Will holding my baby to sleep create bad habits?
In the early weeks, no. Newborns are too young to form ingrained sleep habits, so contact naps won’t “spoil” them. Around three to four months, as babies develop more mature sleep cycles, they can begin to rely on being held to fall asleep, which becomes a sleep association. Even then, the bigger question is whether the baby can regulate on their own. If they physically can’t settle without help, that points to a nervous system issue, not a discipline issue.
Why does my baby wake up the moment I put them down?
Most babies wake on transfer because of the Moro (startle) reflex and immature sleep cycles—the change from warm, supported arms to a cool, flat surface triggers a startle, and they’re often in light sleep when set down. For some babies, frequent and violent startles reflect a nervous system stuck on high alert. If your baby startles intensely at small changes and rarely sleeps deeply, it’s worth assessing how well their Autonomic Nervous System is regulating.
Could birth trauma be why my baby won’t sleep unless held?
It can be a contributing factor. Birth interventions like C-section, forceps, vacuum extraction, or prolonged labor can strain a baby’s upper neck and brainstem, the area where the vagus nerve exits and where sleep-calming pathways concentrate. This can leave the nervous system tilted toward fight-or-flight, making deep, independent rest harder. A neurological assessment can help determine whether birth-related tension is affecting your baby’s ability to settle.
When should I worry about my baby’s sleep?
Reach out to a trusted pediatric provider if your baby sleeps only in very short stretches and never seems rested, has a high-pitched or inconsolable cry, arches or stiffens frequently, struggles to feed, or shows signs of reflux, colic, or constipation alongside sleep troubles. This cluster suggests the nervous system is dysregulated rather than simply immature and deserves a proper evaluation.
Can chiropractic care really help my baby sleep better?
Many families report that gentle, Neurologically-Focused Chiropractic Care helps their baby settle more easily and sleep longer once nervous system interference is reduced and parasympathetic regulation improves. Care begins with a neurological assessment to identify whether the baby is stuck in sympathetic dominance. It’s not a guaranteed cure, and results vary by child, but for babies whose sleep struggles stem from dysregulation, addressing the root cause can make a meaningful difference.



