

If your child struggles with intense fears of movement or falling, they may be experiencing gravitational insecurity, a condition where typical movements trigger intense fear that’s completely out of proportion to any actual danger. This isn’t about a child being cautious or needing encouragement to “be brave.” It’s a real neurological issue affecting how their nervous system processes movement and spatial information.
Here’s what most parents don’t realize: gravitational insecurity isn’t a behavioral quirk your child will outgrow. It’s not a discipline problem, and it’s not in their head. It’s a sign of deeper nervous system dysfunction, specifically, a vestibular system stuck in a heightened state of alarm, constantly sending danger signals when there’s no real threat.
While traditional approaches focus on helping kids cope with these fears through desensitization and accommodation, there’s a different path, one that addresses why their nervous system is stuck in this state in the first place. In this article, we’ll walk you through what gravitational insecurity really is, why it develops, and how addressing the root neurological dysfunction can help your child move from fear to confidence.
What is Gravitational Insecurity?
Gravitational insecurity is an excessive fear of movement, changes in head position, or having feet leave the ground, movements that wouldn’t typically threaten most children. Dr. A. Jean Ayres, who pioneered sensory integration theory, first coined the term in the 1970s.
For a child with gravitational insecurity, that basic sense of security isn’t there. Their nervous system interprets routine movements as dangers, triggering an intense fight-or-flight response. This goes beyond normal cautiousness; these kids experience genuine panic.
Research shows that gravitational insecurity affects 15-21% of children with Sensory Processing Disorder. It’s often dismissed as anxiety or clinginess, but these kids aren’t being difficult. Their vestibular system, responsible for detecting movement and gravity, is dysregulated, sending faulty danger signals to the brain.
At PX Docs, we see gravitational insecurity as a red flag indicating deeper nervous system dysfunction. When a child’s vestibular system is this overreactive, their nervous system is stuck in a heightened state of alert, and that dysregulation doesn’t just affect movement.
The Vestibular System is Your Child’s Internal GPS
The vestibular system starts in the inner ear, where tiny structures detect every movement your child makes. Three semicircular canals track rotation, while the utricle and saccule detect linear movement and gravity itself.
These inner ear sensors send signals to the vestibular nuclei in the brainstem, which process this information alongside vision and proprioception (position sense from muscles and joints) to create an accurate picture of where the body is and how it’s moving.
The vestibular system is one of the first to mature, nearly fully formed by 25 weeks of pregnancy. This early development makes sense given its fundamental nature. You can’t develop motor skills, coordination, or balance without a properly functioning vestibular system as the foundation.
Here’s the critical piece most don’t know: the vestibular system is modulated by proprioceptive input from the upper cervical spine, specifically C1, C2, and C3 at the very top of the neck. When that upper cervical proprioception is distorted (often from birth trauma and subluxation), the vestibular system loses its calibration. It’s like using a GPS with faulty satellite signals; the system gets confused, overreacts to normal movement, and sends alarm signals when there’s no danger.
Recognizing Gravitational Insecurity in Your Child
Gravitational insecurity shows up differently by age, but the common thread is fear responses that are out of proportion to the actual situation.
- In Infancy: Extreme distress during diaper changes or bath time (when head tilts back), difficulty with tummy time, crying when moved from upright to horizontal, preferring to sleep at an incline rather than flat, resisting being picked up.
- In Toddlerhood: Refusing slides or showing panic on them, avoiding climbing playground equipment, taking much longer than peers to master stairs (insisting on holding hands), extreme clinginess in new environments, disliking swings or rocking toys, and walking cautiously on uneven surfaces.
- In School-Age Children: Avoiding playground equipment entirely, refusing to participate in PE or sports, expressing extreme fear of heights, needing both feet on the ground at all times, experiencing motion sickness easily, being labeled “not athletic” when the real issue is fear.
- The Daily Life Impact: Getting dressed becomes difficult because lifting legs challenges balance. Sitting in chairs, especially tall ones, creates anxiety. Car seats feel restrictive. Physical play feels dangerous rather than fun. These kids often become controlling of their environment or rigid about routines because predictability helps them feel safer. What looks like anxiety or behavioral issues is actually a nervous system desperately trying to maintain safety in a body that doesn’t feel secure.
What Causes Gravitational Insecurity?
Most explanations stop at “vestibular dysfunction” without digging into why the vestibular system isn’t working properly. That’s like diagnosing a car problem as “the engine isn’t working” without figuring out what’s wrong with the engine.
Traditional approaches attribute gravitational insecurity to chronic ear infections affecting inner ear structures, delayed vestibular development, sensory processing differences, or premature birth. These factors can play a role, but they don’t explain why so many children with gravitational insecurity share a specific pattern: difficult births, early physical tension (colic, torticollis, head preference), and signs of nervous system dysregulation that go beyond just vestibular signs.
The Missing Piece
The vestibular system is heavily modulated by proprioceptive input from the upper cervical spine. The vertebrae at the very top of the neck have some of the highest concentrations of proprioceptive sensors in the entire body. These sensors constantly feed information to the vestibular nuclei in the brainstem, helping calibrate and regulate the vestibular system’s response to movement.
When there’s dysfunction in these upper cervical segments, tight muscles, restricted joint movement, and abnormal tension patterns, the proprioceptive signals become distorted. It’s like static on a radio signal. The vestibular nuclei aren’t getting clear, accurate information about head and neck position, so they can’t properly process the movement information coming from the inner ear. The result: the vestibular system overreacts, interpreting normal movement as a threat.
Research published in Frontiers in Pediatrics demonstrated this connection directly. The study evaluated 120 colicky babies using a five-point clinical index of vestibular hyperactivity. Before care, colicky babies scored an average of 2.88 on vestibular dysregulation compared to just 0.37 for non-colicky babies, an 87.2% difference. When researchers gently supported the tight upper cervical musculature in these infants, vestibular scores decreased by 96.5%, showing dramatic improvement in how the babies tolerated movement.
The key finding: vestibular dysregulation in these infants wasn’t a problem with the inner ear itself. It was a problem with how upper cervical dysfunction was disrupting the sensory signals that modulate the vestibular system. Fix the upper cervical problem, and the vestibular system can recalibrate.
Birth Trauma’s Hidden Impact
Even “normal” births place significant physical stress on an infant’s upper neck. The baby’s head and neck must rotate, extend, and compress to navigate the birth canal. C-sections involve pulling forces that strain the upper cervical spine. Interventions like forceps, vacuum extraction, or prolonged labor with persistent pushing can all create upper cervical dysfunction.
For most newborns with upper cervical misalignment, the body compensates. But for some, especially with additional stressors, this early trauma creates lasting dysfunction. These are the babies who had difficulty latching, developed a head preference, struggled with colic that seemed neurological rather than digestive, showed asymmetric posture, or had delayed motor milestones.
These early signs often evolve into gravitational insecurity as the child grows, with the vestibular system never properly calibrating.
The “Perfect Storm” of Factors Leading to Gravitational Insecurity
At PX Docs, we use the “Perfect Storm” framework to understand how nervous system issues develop. It’s not one single cause; it’s a combination of stressors during critical windows that overwhelm the developing nervous system.
- Prenatal Stress: When a mother experiences significant stress during pregnancy, stress hormones like cortisol cross the placenta and affect fetal nervous system development. High prenatal stress is associated with increased sensory sensitivity and a nervous system prone to reactive, vigilant states.
- Birth Interventions and Trauma: Birth is often the key physical stressor creating upper cervical dysfunction. Traction, compression, and twisting forces, especially during complicated births, strain the delicate structures of the upper neck. Even “typical” hospital births with epidural, Pitocin, and coached pushing create enough physical stress to impact the upper cervical spine, leading to subluxation.
- Early Childhood Stressors: Persistent colic or reflux, recurrent ear infections and antibiotics, disrupted sleep, delayed motor development, and chronic illness all add to the total load. When the foundation is already shaky from birth trauma, these stressors push the system into chronic dysregulation.
The cumulative effect explains why some children develop gravitational insecurity while others don’t. It’s about the accumulation of multiple stressors during sensitive developmental windows, each one preventing the nervous system from establishing healthy function.
Gravitational Insecurity and Related Conditions
Gravitational insecurity rarely exists alone; it’s often part of a broader pattern of nervous system dysregulation.
- Autism Spectrum Disorder: Research shows that approximately 90% of children with Autism have significant sensory processing challenges, and gravitational insecurity is particularly common. Many experienced the same “Perfect Storm” elements of prenatal stress, birth trauma, gut issues, and persistent dysautonomia.
- ADHD: Children with ADHD often show vestibular seeking behaviors, constant movement, spinning, and rocking. Some show both patterns at different times. The prefrontal cortex (central to attention) has direct connections to the vestibular nuclei, so vestibular dysfunction disrupts attention and impulse control.
- Sensory Processing Disorder: Gravitational insecurity is considered a vestibular-based sensory modulation condition. Children with it almost always have sensory challenges in other areas: tactile defensiveness (bothered by clothing textures), auditory sensitivity (covering ears), visual sensitivity (bright lights), oral sensitivity (extreme picky eating), and proprioceptive seeking (crashing, jumping). This clustering isn’t a coincidence; when upper cervical dysfunction disrupts brainstem function, it affects sensory processing globally.
At PX Docs, we see this constantly: the child comes in for one issue, and we find gravitational insecurity, sensory challenges, sleep problems, digestive issues, and emotional regulation difficulties all in play. It’s a nervous system dysregulated at its foundation.
Traditional Care Approaches for Gravitational Insecurity
Most children with gravitational insecurity work with occupational therapists trained in sensory integration. These therapists use gradual exposure to movement using suspended equipment (swings, bolster swings), starting with minimal challenge and slowly increasing difficulty. They combine vestibular input with proprioceptive activities and create child-directed play that allows control over movement speed and intensity.
Physical therapists use specific vestibular exercises: balance beam walking, ball activities, controlled spinning, and visual-vestibular integration exercises. Many therapists teach accommodation strategies like weighted vests, sensory diets, modified environments, and self-regulation techniques.
These approaches can be extremely helpful; they help children manage dysregulation and gradually build tolerance. The limitation: they’re all compensatory. They help the child cope with a dysregulated vestibular system, but don’t address why it’s dysregulated. They can’t fix the upper cervical dysfunction disrupting proprioceptive signals to the vestibular nuclei. Many children improve with consistent therapy, but progress often plateaus, and they may always need accommodation.
Addressing Gravitational Insecurity at Its Source
We start with a fundamental question: why is this child’s vestibular system dysregulated? We’ve found that addressing the neurological foundation, specifically, the upper cervical spine’s role in modulating the vestibular system, often creates changes that go beyond what traditional therapy alone can achieve.
Neurologically-Focused Chiropractic Care is different from typical chiropractic care. We’re not trying to “crack” your child’s back or force bones into place. Instead, we use precise, incredibly gentle adjustments specifically designed for pediatric neurology. The adjustments we use on children, especially infants and toddlers, involve no more pressure than you’d use to check a tomato for ripeness.
We focus on the upper cervical spine when necessary—those critical C1, C2, and C3 segments where proprioceptive sensors are constantly sending information to the vestibular nuclei. When there’s restriction, tension, or fixation in these segments, that proprioceptive input becomes distorted and the vestibular system loses its calibration.
Gentle, specific adjustments restore normal motion and release suboccipital muscle tension. This allows proprioceptive signals to normalize, which in turn allows the vestibular system to recalibrate. The nervous system can finally receive accurate information about head position and movement, and the overreactive fear response begins to settle.
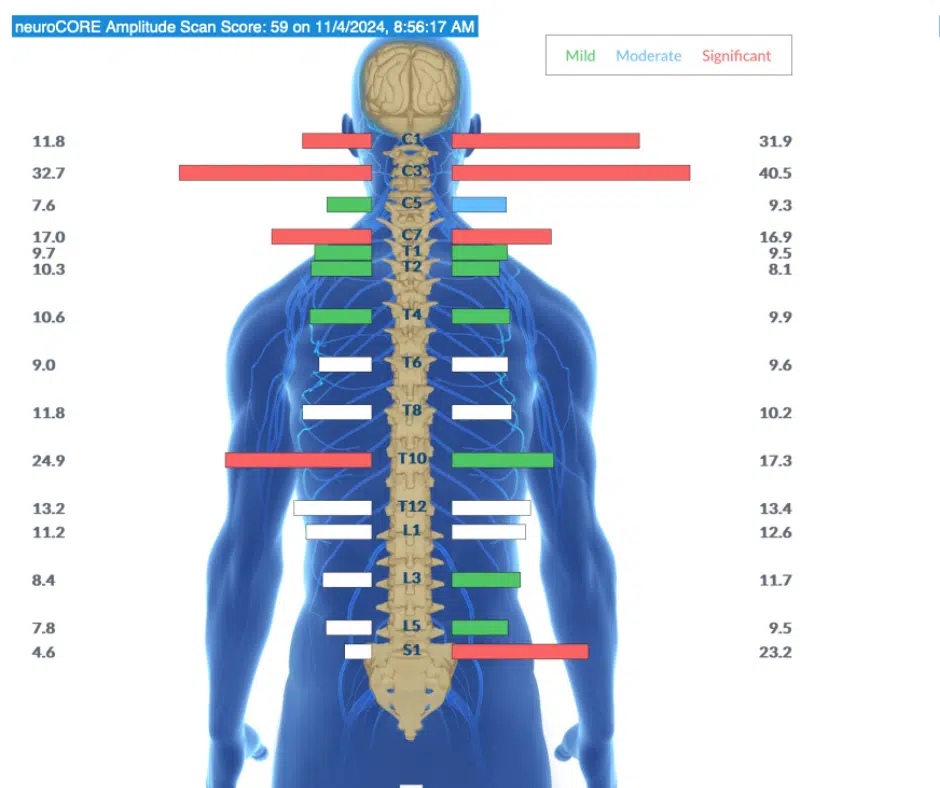
INSiGHT Scanning provides an objective assessment of the nervous system before any adjustment is made. These non-invasive scans measure three critical aspects:
- Thermal Scan: Maps temperature patterns showing where the Sympathetic Nervous System is overactive
- Surface EMG: Measures muscle electrical activity, showing tension, asymmetry, and areas of subluxation
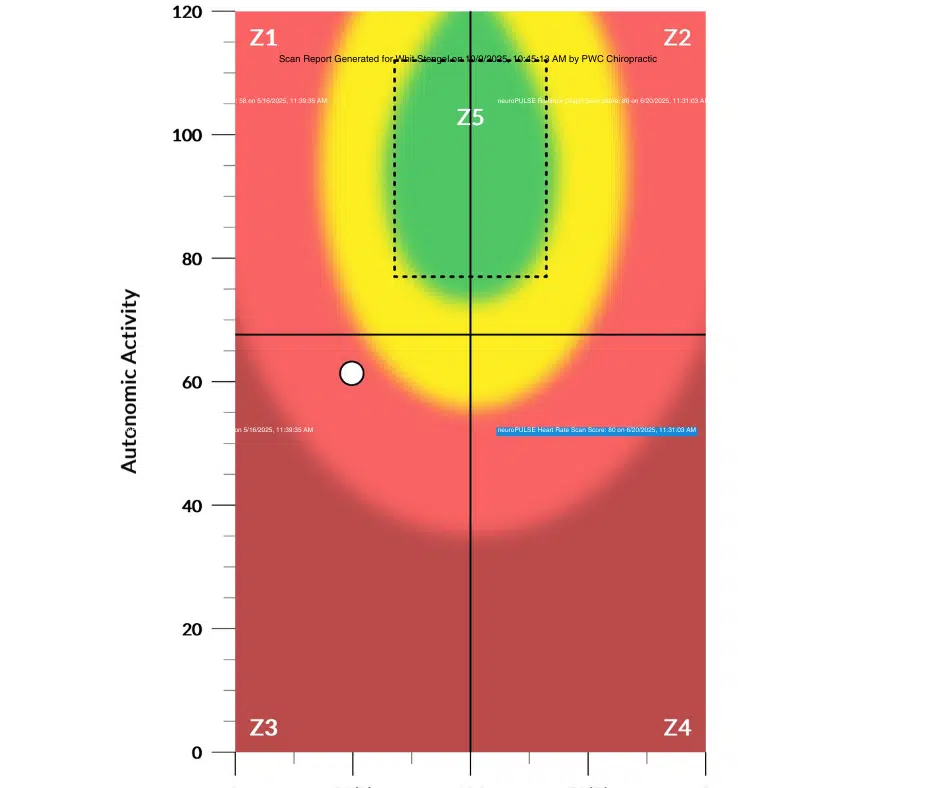
- Heart Rate Variability: Measures the balance between sympathetic (“gas pedal”) and parasympathetic (“brake pedal”) nervous system function
For children with gravitational insecurity, we typically see a distinct pattern: high sympathetic tone in the upper cervical region, increased suboccipital muscle tension, and poor heart rate variability, indicating limited nervous system regulatory capacity. These scans give us an objective picture of the dysfunction underlying the behavioral signs, and they allow us to track progress—watching the nervous system shift from chronic stress to better regulation.
Supporting Your Child with Gravitational Insecurity
- Respect Their Fear: Your child’s fear is real; their nervous system is genuinely signaling danger. Pushing beyond tolerance adds stress to an already dysregulated system. Validate their experience.
- Provide Gradual, Child-Led Exposure: Let them approach new movement experiences at their own pace. If they watch other kids for weeks before trying, that’s okay.
- Offer Heavy Work: Proprioceptive input is calming. Pushing/pulling heavy objects, carrying items, animal walks, jumping, tight hugs, or wearing weighted vests help the nervous system feel grounded.
- Create Predictability: Warn before transitions, explain what’s happening, and offer choices when possible.
- Seek Professional Help If: Gravitational insecurity significantly impacts daily life, shows regression, other developmental red flags appear, traditional approaches have plateaued, or you suspect deeper neurological dysfunction needs addressing.
Moving Forward with Hope
If you’ve watched your child struggle with fears other parents can’t understand, here’s what you need to know: gravitational insecurity isn’t a life sentence. It’s a sign that your child’s nervous system is working with distorted information, stuck in a dysregulation pattern that often began at birth.
Traditional approaches help children cope and build tolerance. But addressing the root cause, the upper cervical dysfunction disrupting proprioceptive signals to the vestibular system, creates a different kind of change. This is about helping the nervous system shift out of the state that created the fear.
We see this regularly at PX Docs: children who couldn’t walk down stairs without panic are now running on playgrounds. Toddlers who screamed during diaper changes are enjoying tummy time. Teens who avoided physical activity are trying out for sports teams.
Your child deserves to feel safe in their own body. With the right support, addressing the right foundation, that’s absolutely possible.To find a PX Docs provider near you, we encourage you to visit our directory.



