

Your child suddenly starts clearing their throat constantly. Or making a repetitive sniffing sound. Maybe it’s a high-pitched squeaking noise that comes out of nowhere. You ask them to stop. They try. They genuinely can’t.
That helplessness, yours and theirs, is one of the hardest parts of watching vocal tics in children. And if you’ve already been through the pediatrician visit only to hear “it’ll probably go away on its own,” you’re likely looking for something more.
This article covers what vocal tics actually are, why they happen, what conditions they’re connected to, and, most importantly, what’s going on in your child’s nervous system that mainstream medicine often doesn’t explain. You’ll also learn what Neurologically-Focused Chiropractic Care looks at that conventional approaches typically miss.
What Are Vocal Tics in Children?
Vocal tics are sudden, involuntary sounds that a child makes repeatedly. They’re not a choice. The child isn’t doing it for attention or out of a habit we normally think of. They’re neurological in origin, meaning the signal is coming from the brain, not from a decision.
Research shows that tics are the most common movement disorder in children, with onset most often between ages 3 and 8. Up to 20% of school-age children will experience some type of tic at some point during childhood.
Many parents first notice vocal tics during periods of increased stress, fatigue, or excitement in their child’s life, such as a new school year, illness, or a big change at home. This timing isn’t random, and we’ll get into why shortly.
The important distinction most parents don’t know: vocal tics and motor tics are different expressions of the same underlying neurological process.
- Motor tics involve involuntary movements such as blinking, shoulder shrugging, and head jerking.
- Vocal tics involve involuntary sounds.
Many children have both at different times, though not always simultaneously.
Simple vs. Complex: The Two Types of Vocal Tics
Not all vocal tics look (or sound) the same. Clinicians divide them into two categories.
Simple vocal tics involve a single, brief sound with no linguistic meaning. These are the most common and include:
- Repetitive throat clearing
- Sniffing or snorting
- Grunting
- Squeaking or squealing
- Coughing without an underlying illness
Complex vocal tics involve more elaborate vocalizations that can include words, phrases, or specific patterns:
- Repeating words or phrases out of context (echolalia or palilalia)
- Animal sounds
- Shouting or yelling
- In rare cases, involuntary use of profanity or socially inappropriate phrases, a phenomenon called coprolalia, which studies indicate affects only about 10% of children with vocal tics, not the majority, as popular culture often implies
Simple vocal tics usually appear first. If complex tics develop, it’s typically later in the progression and often indicates a more established nervous system pattern at work.
What’s Actually Causing Vocal Tics? The Nervous System Explanation
Conventional medicine describes vocal tics as a neurological condition, and that part is accurate. Where it often falls short is explaining why the nervous system is producing these signals in the first place.
Here’s what the research tells us.
Vocal and motor tics originate from disrupted signaling in the basal ganglia, a group of structures deep in the brain that act as the brain’s motor “traffic control.” The basal ganglia constantly filter movement signals, deciding which motor programs to execute and which not to. When these circuits are dysregulated, signals that should be filtered out get through, producing tics.
A 2023 review published in Behavioral Sciences found that the origin of tic conditions is multifactorial, with strong genetic, perinatal, and immunological influences. It’s not just genes. It’s the cumulative load on a developing nervous system.
The key neurotransmitter involved is dopamine. Think of dopamine as the brain’s “gas pedal”; it drives movement signals forward. In children with tic disorders, research consistently shows dysregulated dopamine activity in the striatum (part of the basal ganglia), creating a state where the brake pedal, controlled largely by GABA and the Parasympathetic Nervous System, can’t keep up with the accelerator. Research published in PMC confirms that excess striatal dopamine excites thalamocortical circuits that produce tics, and that emotional stressors amplify this through the HPA axis.
This is important: the HPA axis is the body’s central stress response system. When a child’s Autonomic Nervous System is stuck in a chronic sympathetic “fight-or-flight” state, what we call sympathetic dominance, the HPA axis stays activated. That means more cortisol, more dopamine dysregulation, and more tic activity. Stress doesn’t just trigger tics. For many children, a dysregulated nervous system is what makes them vulnerable to tic disorders in the first place.
Why Tics Wax and Wane: The Triggers Parents Notice
If you’ve watched your child’s tics for any length of time, you’ve probably noticed they’re not constant. They come and go. They get worse at certain times and quiet down at others.
This waxing and waning pattern is a hallmark of tic disorders. And the triggers parents report most consistently make complete neurological sense:
- Stress and anxiety amplify tics because they push the nervous system further into sympathetic dominance, flooding the striatal circuits with dopamine. The HPA axis goes into overdrive, and the basal ganglia loses even more of its filtering capacity.
- Fatigue and poor sleep reduce the prefrontal cortex’s ability to exert inhibitory control over the basal ganglia pathways. Sleep deprivation essentially removes one of the brain’s last natural brakes on tic activity. A 2025 study found that children with Tourette’s syndrome face a significantly elevated risk of sleep disorders, suggesting the nervous system dysregulation behind tics directly affects sleep architecture.
- Excitement, even positive excitement like a birthday party or holidays, can spike tic activity because it triggers the same sympathetic arousal response as stress. The nervous system doesn’t distinguish between “exciting” and “scary.”
- Illness and infection stress the immune system and can temporarily increase neuroinflammation, pushing already-sensitive basal ganglia circuits into greater dysregulation.
- Talking about or focusing on tics notoriously makes them worse. This isn’t a behavioral quirk; it’s because focused attention on tics increases cortical activation in areas that feed directly into the basal ganglia loop.
Types of Tic Disorders: What the Diagnoses Actually Mean
When vocal tics persist, a doctor may diagnose one of three main tic conditions. The distinction comes down to duration and whether motor tics are also present.
- Provisional Tic Disorder (formerly called transient tic disorder) is the most common diagnosis, particularly in younger children. A child has motor or vocal tics, or both, for less than one year. This affects up to 10% of school-age children. Most cases resolve without formal treatment.
- Persistent (Chronic) Tic Disorder means a child has had either motor or vocal tics (not both simultaneously) for more than 12 months. Less common than provisional tic disorder, this affects less than 1% of school-age children.
- Tourette’s syndrome is diagnosed when a child has two or more motor tics and at least one vocal tic, lasting more than one year, with onset before age 18. Contrary to the stereotype, most children with Tourette’s syndrome do not have coprolalia. The condition exists on a spectrum of severity; many children with Tourette Syndrome lead full, unimpaired lives with the right support.
One additional pattern worth knowing: some children develop sudden, severe tic onset or dramatic worsening following a streptococcal infection. This is associated with PANDAS/PANS, where antibodies produced against the strep infection cross-react with basal ganglia tissue. If your child’s tics appeared seemingly overnight after strep throat, this connection is worth discussing with a knowledgeable provider.
What Conditions Travel With Vocal Tics
Vocal tics rarely show up in isolation. The same nervous system dysregulation that drives tic activity often affects multiple regulatory systems simultaneously. Parents should know that the following co-occurring conditions are extremely common, not coincidental:
- ADHD is a frequently co-occurring condition with tic disorders. Both involve dysregulation of dopamine and norepinephrine pathways, and the same basal ganglia-prefrontal circuits that struggle to filter out tics also struggle to maintain sustained attention and impulse control.
- OCD shares neurological circuitry with tic disorders, particularly the cortico-striato-thalamo-cortical (CSTC) loop. The intrusive, repetitive nature of OCD compulsions mirrors the compulsive quality of tics, that feeling of a building urge that only resolves by completing the action.
- Anxiety is both a co-occurring condition and a trigger. A child whose nervous system stays in chronic sympathetic overdrive will experience anxiety as a baseline state, not just as situational stress. The vagus nerve, the primary parasympathetic highway connecting the brain to the body, plays a direct role here. When the vagus nerve is underactive or impaired, the calming “brake” on the nervous system simply doesn’t work well, leaving anxiety and tic activity to reinforce each other.
- Sensory Processing challenges frequently overlap with tic disorders. The same dysregulated brainstem processing that creates sensory overwhelm can contribute to the heightened neural sensitivity that makes tics more likely.
- Sleep disruption is both a trigger and a consequence. Poor sleep worsens tic severity; tic activity (especially at night) disrupts sleep quality.
Why Conventional Treatment Often Misses the Root Cause
The standard treatment options for vocal tics in children are behavioral therapy and medication.
Comprehensive Behavioral Intervention for Tics (CBIT) is one approach. It teaches children to recognize the premonitory urge before a tic, identify high-risk situations, and practice a competing response behavior that physically blocks the tic.
CBIT is genuinely useful; it’s not a dismissal to say that it’s also a management strategy rather than a root-cause solution. It trains children to work around dysregulated nervous system signals. It doesn’t address why those signals are dysregulated in the first place.
Medication, primarily neuroleptics (antipsychotics) and alpha agonists, works by dampening dopamine activity in the basal ganglia or reducing sympathetic arousal. These can reduce tic frequency and intensity for some children. The trade-offs include sedation, weight changes, and the fact that tics often return when medication is discontinued, because the underlying dysregulation hasn’t been addressed.
What both approaches leave unasked: Why is this child’s nervous system producing these signals? Why is the brake pedal not working? Why is the basal ganglia stuck in this pattern? For many children, that answer traces back further than the tics themselves, back to how the nervous system developed in the first place.
The “Perfect Storm”: Why Some Children Develop Tic Disorders
At PX Docs, we talk a lot about the “Perfect Storm,” the combination of early-life stressors that can overwhelm a developing nervous system and leave it stuck in patterns of dysregulation that show up later as tic disorders, ADHD, anxiety, or sensory challenges.
The Perfect Storm typically involves three converging factors:
1. Preconception & Prenatal Stress: Prenatal stress and maternal anxiety during pregnancy expose the developing fetus to elevated cortisol and stress hormones that cross the placenta. This can shape the basal ganglia and dopaminergic circuits before a child is even born, essentially programming the nervous system toward a state of sympathetic dominance before birth. Research confirms a significant association between maternal autoimmunity and inflammatory states during pregnancy and childhood tic onset.
2. Birth Trauma and Interventions: Birth trauma, including but not limited to forceps or vacuum-assisted delivery, prolonged labor, c-section, induction, manual assistance, or cord entanglement, creates physical stress to the infant’s upper neck, brainstem, and vagus nerve. This region, the craniocervical junction, is the most neurologically critical part of the spine during infancy. Physical tension or subluxation here disrupts the normal flow of sensory information between the body and brain, creating an altered neurological baseline that can affect basal ganglia function and sympathetic/parasympathetic balance.
3. Early Childhood Stressors: Colic, reflux, recurrent ear infections, frequent antibiotics, environmental toxins, food sensitivities, chronic illnesses; these aren’t just “normal baby stuff.” Each one adds strain to an already-taxed developing nervous system. When the neuro-immune system gets hit repeatedly before it’s had a chance to establish healthy regulation, the result is chronic nervous system dysregulation, the kind that shows up later as tics, anxiety, sensory overload, and attentional difficulties.
None of this means tics are inevitable with a difficult birth or a stressful pregnancy. But it helps explain why some children develop tic issues, while others don’t, and, more importantly, points toward what could actually be addressed at the root level.
Neurologically-Focused Chiropractic Care and Vocal Tics
Neurologically-Focused Chiropractic Care doesn’t treat or cure tic conditions. It doesn’t diagnose them or prescribe for them. What it does is assess and address the underlying nervous system dysregulation that we believe sets the stage for tic activity to develop and persist.
The specific focus is subluxation, neurological interference in the spine and brainstem that disrupts proper communication between the brain and body. In children, subluxation most commonly results from the physical stressors of birth and early childhood, and it tends to drive the nervous system toward sympathetic dominance: the gas pedal stuck down, the brake pedal suppressed.
When subluxation is present, the vagus nerve, which runs from the brainstem down through the neck and into the organs, can’t function the way it should. Vagus nerve dysfunction impairs the parasympathetic response, reducing the body’s natural capacity to down-regulate stress, calm the HPA axis activity, and restore the dopaminergic balance that the basal ganglia needs to properly filter motor signals.
Chiropractic adjustments, in this context, aren’t about back pain. They’re about reducing neurological interference, supporting the vagus nerve’s tone, and helping the Autonomic Nervous System find its way back toward balance. When the brake pedal starts working better, many families report that their children are calmer, sleep better, have fewer sensory triggers, and for some, tic frequency and intensity decrease as the nervous system regulation improves.
This isn’t a promise of a cure or a replacement for established care. It’s an essential layer that addresses something CBIT and medication simply don’t reach: the foundational nervous system state driving the pattern.
Seeing the Nervous System Behind the Tics with INSiGHT Scans
One of the tools PX Docs practitioners use is INSIGHT scanning technology, a neurological assessment tool that objectively measures Autonomic Nervous System function without relying solely on symptoms.
The INSiGHT scan uses three components:
- A surface EMG to assess neuromuscular tension and nerve interference along the spine
- A thermal scan to measure autonomic asymmetry (how well the nervous system is regulating circulation and temperature)
- Heart rate variability (HRV) to assess the balance between sympathetic and parasympathetic function, and how well your child’s body is adapting to stress
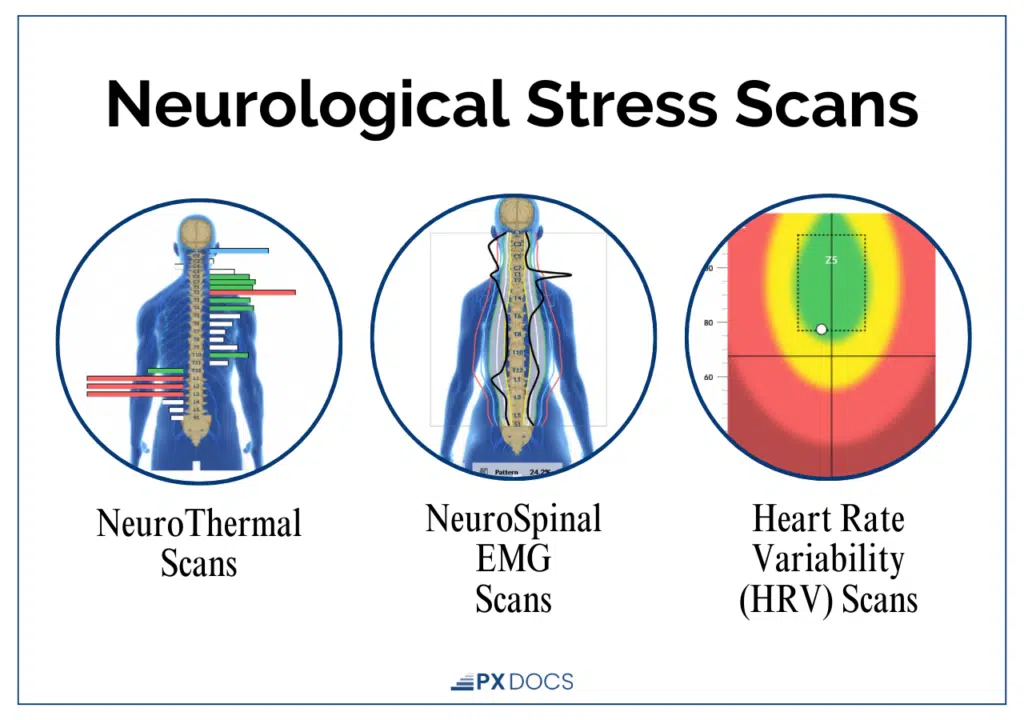
For children with vocal tics, these scans often reveal clear patterns of sympathetic dominance, reduced vagal tone, and neurological disorganization, even when the child appears relatively calm on the surface. This gives families something concrete to look at, not just a symptom checklist.
Important to note: INSiGHT scanning does not diagnose tic disorders, treat any condition, or cure or prevent any health challenge. What it does is provide an objective window into the nervous system’s regulatory state, revealing the patterns that may be contributing to why tics are present and persistent.
What Parents Can Do Now
If your child has vocal tics, here’s what’s worth keeping in mind: don’t panic. Most tics in younger children, especially those present for under a year, resolve on their own. Drawing excessive attention to tics can actually increase them, so a calm, matter-of-fact response at home matters.
Always, take the nervous system seriously. Track when tics are better and worse. Sleep quality, stress load, illness, dietary changes, these patterns tell you something real about your child’s neurological state.
If you’re ready to explore whether Neurologically-Focused Chiropractic Care might be a fit for your child, find a qualified provider in the PX Docs directory. A trained practitioner can perform an INSiGHT scan, take a thorough developmental history, and help you understand what’s happening in your child’s nervous system, not just what’s visible in their symptoms.
Your child isn’t broken. Their nervous system is asking for support.



