

ARFID (Avoidant/Restrictive Food Intake Disorder) is a recognized eating disorder in the DSM-5 characterized by persistent avoidance of food due to sensory sensitivity, fear of negative consequences, or lack of interest in eating, leading to nutritional deficiencies, weight loss, and impaired daily functioning in children. Unlike anorexia or bulimia, ARFID has nothing to do with body image and affects an estimated up to 5% of children.
As a parent, you’ve probably heard it all: “They’ll eat when they’re hungry,” “it’s just a phase,” or “all kids are picky eaters.” But deep down, you know that what your child is going through goes far beyond a preference for chicken nuggets over broccoli. When mealtimes become a source of anxiety, tears, and conflict, and your child’s diet has narrowed to just a handful of “safe” foods, you’re dealing with something much more significant than typical childhood pickiness.
For many children, it’s rooted in nervous system dysregulation that makes eating genuinely difficult, uncomfortable, or even painful.
What Is ARFID in Children?
ARFID stands for Avoidant/Restrictive Food Intake Disorder, and it was officially added to the DSM-5 in 2013, in which children avoid or restrict food intake severely enough to cause nutritional deficiencies, significant weight loss, dependence on supplements, or interference with daily functioning.
ARFID has nothing to do with body image. Instead, children with ARFID avoid food for reasons related to sensory sensitivity, fear of negative consequences like choking or vomiting, or a genuine lack of interest in eating.
What makes ARFID different from typical picky eating is the severity. A picky eater might turn their nose up at vegetables, but still grow normally. A child with ARFID may eat so few foods that they experience nutritional deficiencies, significant weight loss, dependence on supplements, and interference with daily functioning.
Many pediatricians aren’t trained to identify ARFID, and even with a diagnosis, if appropriate, families are often left without answers about what’s actually driving it.
What Are the Signs and Symptoms of ARFID in Children?
ARFID in children generally presents through three distinct profiles, and a child may show features of more than one:
The first is sensory-based avoidance, where children gag, retch, or vomit in response to specific textures, smells, colors, or temperatures of food. They have extremely rigid preferences, and new foods can trigger genuine panic.
The second is fear-based avoidance, often developing after a traumatic experience like choking or an allergic reaction. These children may become terrified of swallowing or restrict intake to only foods they believe are “safe.”
The third is a lack of interest in eating, in which children forget to eat, feel full after a few bites, or simply don’t experience hunger as usual. This presentation is often connected to nervous system dysregulation that disrupts signals for hunger and satiety, controlled by the vagus nerve.
Common Signs Of Arfid Include:
- Poor weight gain or weight loss: falling off growth curves despite adequate food availability
- Extreme food selectivity: consistently eating fewer than 20 foods
- Gagging or retching: physical reactions to new textures, smells, or food appearances
- Mealtime distress: regular meltdowns, crying, or anxiety around eating
- Fatigue and difficulty concentrating: from inadequate nutritional intake
- Delayed growth: falling behind developmental milestones
- Frequent illness: weakened immune function from nutritional gaps
- Stomachaches and constipation: signs of underlying digestive and nervous system dysfunction
These signs often appear across multiple body systems simultaneously because ARFID affects the nervous system, the master control system that coordinates digestion, sensory processing, and emotional regulation.
The Nervous System Connection Most Doctors Miss
Most conventional resources describe ARFID as a combination of genetics, temperament, negative food experiences, and sensory processing challenges. They’re not wrong, but they’re describing the branches of the tree, not the roots.
Here’s what the conventional conversation misses: the Autonomic Nervous System controls virtually every aspect of eating and digestion. The entire process, from feeling hungry to tolerating the sight and smell of food, to chewing and swallowing safely, to moving food through the digestive tract, is regulated by the nervous system.
The vagus nerve, the primary nerve of the parasympathetic “rest and digest” system, plays a central role. It controls stomach acid production, gut motility, the gag reflex, swallowing coordination, hunger signals, and sensory processing within the mouth and throat.
When the vagus nerve isn’t functioning well, when the nervous system is stuck in sympathetic “fight or flight” mode, your child’s body is literally telling them that eating is dangerous. Not because of a psychological problem, but because the neurological wiring that controls eating is compromised.
This is why so many children with ARFID also struggle with reflux, sensory sensitivities, anxiety, and sleep issues. They’re not separate problems; they’re all connected to the same underlying nervous system dysfunction.
What Conditions Commonly Co-Occur with ARFID
ARFID rarely exists in isolation. Studies have found that as high as 82% of children with ARFID also deal with a co-occurring psychiatric condition, and the nervous system connection explains why.
Food selectivity has been shown to affect children with Autism, with many meeting ARFID criteria. Children with ADHD struggle with eating because the same sympathetic dominance that drives hyperactivity also disrupts the calm state needed for meals.
Anxiety and ARFID are deeply intertwined, both driven by an overactive sympathetic nervous system, the “gas pedal,” that can’t shift into a calm parasympathetic state. And the connection to Sensory Processing Disorder is perhaps most obvious, as both reflect a nervous system that can’t properly filter and integrate sensory information.
These aren’t separate problems. They’re different expressions of the same neurological roots.
How Does the “Perfect Storm” Lead to ARFID in Children
At PX Docs, we call it “The Perfect Storm,” a predictable sequence of stressors that pushes a child’s nervous system into chronic dysfunction.
- Prenatal stress: It often begins with prenatal stress. Research shows that maternal stress hormones cross the placental barrier and affect the developing baby’s autonomic nervous system. This isn’t about blame; it’s about understanding that a baby’s nervous system may already be set to a higher stress baseline before birth.
- Birth trauma: Then comes birth trauma. C-sections, vacuum extraction, forceps, induction, prolonged labor, and emergency procedures can create physical stress to the baby’s upper cervical spine, brainstem, and cranial nerves, including the vagus nerve. Many parents of children with ARFID can trace feeding difficulties back to infancy, trouble latching, excessive spit-up, colic, or discomfort during feeds. These early signs are often dismissed but can be the first indicators of vagus nerve dysfunction.
- Environmental factors: Finally, the early childhood cascade compounds everything. Rounds of antibiotics destroy gut bacteria essential for digestion. Reflux medications reduce stomach acid. Chronic constipation signals that the nervous system isn’t controlling gut motility. What started as colic becomes reflux, then food sensitivities, then texture aversions, then a diet so restricted it meets ARFID criteria.
As Dr. Tony Ebel often says, “They don’t grow out of it, they grow into it.”
How Neurologically-Focused Chiropractic Care Addresses ARFID
This is where Neurologically-Focused Chiropractic Care offers something genuinely different.
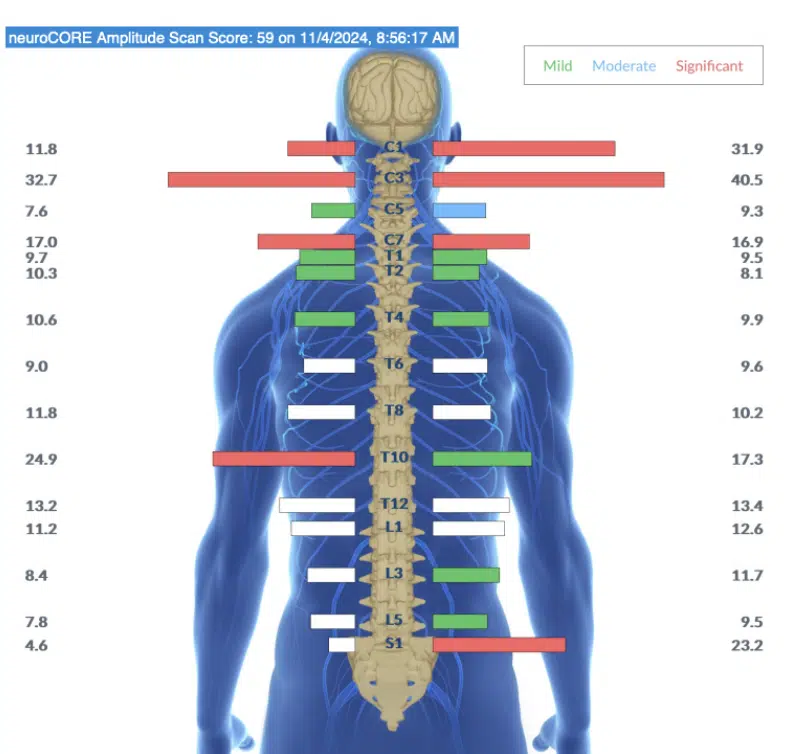
INSiGHT Scanning
Our trained PX Docs use INSiGHT Scanning technology, which includes:
- Heart Rate Variability (HRV) testing to measure autonomic balance and adaptability
- Surface EMG (sEMG) scanning to identify areas of neurological tension along the spine
- Thermal scanning to detect patterns of autonomic dysfunction.
It’s important to note that this technology does not diagnose medical conditions, and Neurologically-Focused Chiropractic Care is certainly not a treatment or cure for ARFID or any other condition, not even back pain. Instead, these INSiGHT Scans help us track down the root cause of nervous system dysfunction and dysregulation, and build customized care plans and adjusting protocols to help shift the nervous system back into a state of balance, regulation, and resilience.
For children with ARFID, these scans frequently reveal significant sympathetic dominance and tension concentrated in the upper cervical area, right where the brainstem and vagus nerve are located.
Addressing Subluxation
At the core of this care is addressing subluxation, which involves misalignment, fixation, and neurological interference that disrupts brain-body communication. When subluxation patterns, especially in the upper cervical spine, are addressed through gentle, specific adjustments, the nervous system can begin shifting out of its stuck sympathetic state.
Parents often report big improvements. First, sleep improves. Then digestion starts functioning better, with constipation resolving and bloating decreasing. As the nervous system continues to regulate, sensory sensitivities decrease, and the child gradually becomes more willing to expand their diet.
Practical Steps for Parents
While addressing the neurological foundation is essential, you can start supporting your child today. Create a calm mealtime environment by turning off screens, reducing noise, and keeping mealtimes low-pressure.
Support vagus nerve function through belly breathing before meals, singing or humming, outdoor play, and prioritizing sleep. Track your child’s nervous system patterns, like sleep quality, bowel function, and overall anxiety, rather than obsessing over food intake alone.
When building your support team, the order matters. Start with the neurological foundation through Neurologically-Focused Chiropractic Care, then layer in feeding therapy, occupational therapy, and nutritional support as the nervous system becomes more regulated. Therapies added onto a stable neurological foundation are far more effective.
Finding Hope and Taking the Next Step
If your child is struggling with ARFID, you’re not imagining it, you’re not overreacting, and you’re not a bad parent. ARFID is real, it’s complex, and it deserves more than a “they’ll grow out of it” response.
But there is tremendous hope. When you address the nervous system dysfunction at its source, real, lasting change becomes possible. Your child’s nervous system is designed to heal, adapt, and grow. Sometimes it just needs the right support to get unstuck.
To find a trained PX Doc in your area, visit the PX Docs Directory. It’s the first step toward real answers.
Frequently Asked Questions About ARFID in Children
Can ARFID in children go away on its own?
ARFID typically does not resolve on its own without intervention. Unlike typical picky eating phases that children outgrow by age 5–6, ARFID involves nervous system dysregulation that drives sensory aversions, fear responses, or lack of hunger signals. Without addressing the underlying autonomic dysfunction, the food restrictions tend to persist or worsen over time. Early intervention that targets both the neurological root cause and behavioral patterns produces the best long-term outcomes.
What is the difference between ARFID and picky eating?
The key difference is severity and impact. Picky eaters may prefer certain foods but still maintain adequate nutrition and normal growth. Children with ARFID eat so few foods that they experience nutritional deficiencies, weight loss, dependence on supplements, or significant interference with daily functioning. ARFID is a diagnosable eating disorder in the DSM-5, while picky eating is a normal developmental phase. If a child consistently eats fewer than 20 foods and mealtimes regularly cause distress, ARFID should be evaluated.
Is chiropractic care safe for children with ARFID?
Neurologically-Focused Chiropractic Care for children uses gentle, precise adjustments specifically calibrated to a child’s size and neurological patterns. It does not diagnose or treat ARFID directly. Instead, it identifies and addresses subluxation and nervous system dysregulation that may be contributing to the sensory sensitivities, digestive dysfunction, and autonomic imbalance underlying many cases of ARFID. INSiGHT Scans provide objective neurological measurements to guide and monitor care.
How long does it take to see improvement in a child with ARFID?
Every child’s timeline is different depending on the severity of nervous system dysregulation. Parents typically report that sleep improves first, followed by better digestion and reduced constipation, then gradual decreases in sensory sensitivities. Meaningful expansion of food variety often takes several months of consistent neurological care combined with appropriate feeding support. Tracking nervous system indicators such as sleep quality, bowel function, and anxiety levels provides a clearer picture of progress than counting only accepted foods.
What causes ARFID in children?
ARFID develops through a combination of nervous system dysregulation, sensory processing differences, and sometimes fear-based responses to negative food experiences. Many cases can be traced to what Dr. Tony Ebel calls the “Perfect Storm”—prenatal stress, birth trauma, and early childhood stressors like antibiotics and illness that overwhelm the developing nervous system. This creates sympathetic dominance and vagus nerve dysfunction, directly impairing digestion, hunger signaling, and the sensory tolerance needed for eating.
Can ARFID cause long-term health problems in children?
Yes. Untreated ARFID can lead to significant nutritional deficiencies, including iron, zinc, and vitamin D deficiency, delayed growth, weakened immune function, bone density problems, and impaired cognitive development. The psychological effects—including increased anxiety around food, social isolation at mealtimes, and family stress—can also compound over time. Addressing ARFID early, particularly the underlying nervous system dysfunction driving it, helps prevent these long-term consequences.



