

Maybe you’ve noticed your child suddenly starts blinking rapidly, clearing their throat every few seconds, or jerking their head to the side, over and over again. They try to stop, but they can’t. Not really.
That moment is terrifying for most parents. And the first question out of almost every parent’s mouth is the same: What’s causing this?
The conventional medical answer, “genetics and changes in the brain”, is somewhat true. But it’s incomplete in a way that matters. Because if you understand why a child’s brain gets stuck in patterns like this, you gain real ground. You understand what’s driving tics, what worsens them, and what might actually help, not just manage them.
This article covers what causes tics in children, what the research says about the neurological mechanisms involved, and why some children are far more prone to developing tics than others.
What Are Tics?
Tics are sudden, repetitive, involuntary movements or sounds that a child produces without meaning to. They’re not habits. They’re not behavioral choices. They’re neurological outputs, the body acting on signals it didn’t consciously generate.
Experts estimate that at least 20% of children will experience a tic at some point, though the real lifetime number may be closer to 75%.
Most parents notice tics first because they look purposeful. A child who blinks rapidly might look like they have something in their eye. A child who repeatedly clears their throat might seem to be developing a cold. A child who shrugs their shoulder over and over might appear distracted. The reality is that none of these are intentional.
One clue that separates tics from ordinary behavior: many children can briefly suppress them. They feel what’s called a premonitory urge, an uncomfortable internal tension that builds until they release it through the tic. Giving in provides momentary relief, similar to finally scratching an itch. But that urge always comes back. And the harder a child tries to hold it in, the worse it gets when it finally releases.
Stress, excitement, fatigue, and illness all tend to make tics more intense. Focused engagement, video games, reading, and sports can sometimes quiet them temporarily. That variability is a feature of how the nervous system governs tic activity, and it’s an important clue to understanding their root cause.
Motor Tics vs. Vocal Tics
All tics fall into one of two main categories:
- Motor tics involve physical movements such as eye blinking, facial grimacing, shoulder shrugging, head jerking, or more complex sequences like hopping or touching objects.
- Vocal tics involve sounds such as throat clearing, sniffing, grunting, or barking, or, in more complex forms, repeating words or phrases. The well-known but rare coprolalia (involuntary swearing) affects less than 15% of those with Tourette syndrome and is not typical of most childhood tic disorders.
Simple tics involve just one muscle group and last less than a second. Complex tics are coordinated patterns across multiple muscle groups. Motor tics tend to appear before vocal tics during development, and both can change location and character over time.
Types of Tic Disorders
Not every child with a tic has a tic condition. Many children experience transient tics—lasting a few weeks to a few months—that may resolve over time, though the underlying factors contributing to them can still be present. When tics persist, they may qualify for one of three formal diagnoses.
- Provisional (Transient) Tic Disorder is the most common. A child has motor tics, vocal tics, or both for less than one year. Research indicates this affects up to 10% of school-age children at some point, and most cases resolve without any intervention.
- Persistent (Chronic) Tic Disorder involves either motor or vocal tics, but not both, lasting longer than one year. This is less common, affecting fewer than 1% of school-age children.
- Tourette Syndrome requires both multiple motor tics and at least one vocal tic, present for more than one year, beginning before age 18. It’s more common than most people think, approximately 1 in 162 school-age children, and it frequently co-occurs with ADHD, OCD, and anxiety.
The distinction between these diagnoses matters less than understanding what’s driving the tics in the first place. And that’s where conventional medicine often stops short.
What Causes Tics in Children: The Conventional Explanation
The standard medical answer points to three converging factors: genetics, neurobiology, and environmental triggers.
Genetics clearly plays a role. Tic conditions run in families. A child with a first-degree relative who has Tourette syndrome or another tic condition is 10 times more likely to develop tics themselves, suggesting inherited patterns in how certain brain circuits are organized and regulated.
The basal ganglia are the neurological structures most consistently implicated in tic production. This cluster of brain structures coordinates motor control, filters out unwanted movements, and helps regulate behavior. When the basal ganglia and the cortico-striato-thalamo-cortical loop (the circuit that governs voluntary motor control) become dysregulated, unwanted movements and sounds break through.
Research consistently shows altered dopamine signaling in these pathways in children with tic conditions; excessive dopaminergic activity in specific regions means the brain’s “filter” doesn’t work as efficiently.
PANDAS (Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections) is worth noting here. In some children, a strep infection triggers an autoimmune response that produces antibodies that mistakenly attack basal ganglia tissue.
This is called molecular mimicry: the antibodies mistake the child’s own brain cells for strep bacteria due to structural similarities. The result can be a sudden, dramatic onset or worsening of tics, OCD behaviors, and other neuropsychiatric signs. PANDAS is more common than the medical mainstream currently recognizes, and it illustrates how powerfully the nervous system and immune system interact.
Environmental triggers, stress, illness, sleep deprivation, certain medications, and in rare cases substances like stimulants, can worsen tics or tip a child over the threshold into a diagnosable tic disorder.
This much is settled science. But it leaves a critical question unanswered: why are two children from similar genetic backgrounds, similar environments, similar stress loads, with one developing tic behaviors and one not?
The Nervous System’s Role
The basal ganglia don’t function in isolation. They’re part of a larger neurological ecosystem, and that ecosystem is regulated, at its deepest level, by the Autonomic Nervous System (ANS).
The ANS has two branches that should work in balance. The Sympathetic Nervous System is the gas pedal; it activates the body in response to stress, threat, or excitement. The Parasympathetic Nervous System is the brake pedal; it slows things down, allows recovery, and enables regulation. When that balance is intact, the brain can properly filter motor signals, manage emotional regulation, and adapt to stress.
When it’s not, when a child’s nervous system is chronically stuck in sympathetic dominance, that balance breaks down. The “filter” that the basal ganglia normally provides becomes less effective. Dopaminergic pathways that regulate motor control become sensitized to stress. The threshold for tic expression drops.
This is why stress so reliably worsens tics. It’s not just psychological. Stress activates the sympathetic nervous system. And in a child already running with the gas pedal stuck down, more sympathetic activation means less ability to filter out unwanted motor and vocal outputs.
The vagus nerve is the body’s primary brake pedal. It’s the longest cranial nerve in the body, running from the brainstem through the neck, chest, and abdomen. Its job is to activate the Parasympathetic Nervous System and regulate everything from heart rate to digestion to inflammation to emotional state. When vagus nerve function is healthy, the nervous system can recover from stress and return to baseline. When vagus nerve function is compromised, the system stays in a constant state of high alert.
Children with tic conditions consistently show patterns of Autonomic Nervous System dysregulation, lower heart rate variability, higher resting sympathetic tone, and impaired recovery from stress. This isn’t a coincidence. It’s the mechanism. The tics are, in many ways, signs of a nervous system that can’t properly regulate itself.
Why Are More Children Developing Tic Disorders Now?
At PX Docs, we use a framework called the “Perfect Storm” to explain why some children develop chronic neurological challenges, including tics, while others with similar genetics and environments don’t.
The “Perfect Storm” describes a sequence of early-life neurological stressors that accumulate and compound, disrupting the developing nervous system in ways that conventional medicine often fails to trace back to their origins.
- Stage 1: Prenatal Stress. The Autonomic Nervous System begins developing in utero. Maternal stress, anxiety, illness, hormone disruption, and toxin exposure during pregnancy all cross the placenta and influence how the fetal nervous system is calibrated from the very beginning. A nervous system that begins development under chronic stress starts life with the sympathetic accelerator already partially engaged.
- Stage 2: Birth Trauma. The upper cervical spine and brainstem region, where the vagus nerve originates, is exceptionally vulnerable during delivery. C-sections, forceps, vacuum extraction, induction, prolonged labor, and rapid delivery all apply forces to this area that can cause birth trauma and subluxation. Subluxation, patterns of neurological interference within the neurospinal system, disrupts the normal flow of signals between the brain and body. When it occurs at the brainstem level, vagus nerve function is directly compromised from the start.
- Stage 3: Early Childhood Accumulation. Colic, reflux, recurrent ear infections, antibiotic exposure, and sleep disruption in the first years of life continue to burden an already stressed system. By the time a child reaches school age, their nervous system has been running in survival mode for years. The gas pedal has been pressed for so long that the brake pedal has barely had a chance to develop.
When a child is built on this neurological foundation and then encounters the ordinary stressors of childhood, school pressure, illness, growth spurts, their system has much less reserve to absorb them. That’s when tics often emerge. Not because of one event, but because the nervous system has finally run out of room to compensate.
What Makes Tics Better or Worse?
The factors that modulate tics aren’t random. They’re a map of the Autonomic Nervous System.
Tics get worse with stress, anxiety, excitement, and illness, all states of heightened sympathetic activation. They often worsen with fatigue because a tired nervous system loses its regulatory capacity even faster. Many parents notice that tics peak after school, when a child has been suppressing them all day, when social pressure to conform is high, and then release them at home.
Tics tend to improve during focused, absorbing activity, video games, sports, and creative work, because these states engage the brain in ways that can temporarily suppress the motor circuits involved. They also tend to improve with relaxation, adequate sleep, and low-stress routines.
Notably, tics often worsen at puberty, then improve in late adolescence and adulthood. This pattern may reflect the profound neurological changes of adolescence, including shifts in dopaminergic signaling, hormonal fluctuations, and ongoing maturation of frontal lobe circuits that regulate basal ganglia output.
The co-occurrence of tics with ADHD, OCD, and anxiety situations isn’t coincidental. All of these share a common neurological substrate: dysregulated cortico-striato-thalamo-cortical circuits, altered dopamine and serotonin signaling, and autonomic imbalance. Caring for only the tics while ignoring the broader nervous system state is like caring for the smoke while leaving the fire.
How Neurologically-Focused Chiropractic Care Approaches Tic Disorders
Conventional care for tics includes behavioral therapies like Comprehensive Behavioral Intervention for Tics (CBIT) and medications such as guanfacine or aripiprazole, which can reduce tic frequency and severity. They’re available tools, and can have their place. But they work at the level of trait management, not root-cause resolution.
Neurologically-Focused Chiropractic Care takes a different starting point. Rather than asking “how do we suppress the tics?”, it asks “what’s happening in this child’s nervous system that’s producing them?”
Neurologically-Focused Chiropractic adjustments work to restore proper neurospinal function, reduce sympathetic dominance, and support vagal tone. The goal isn’t to “treat” tics directly; it’s to restore the neurological balance the body needs to regulate itself. When the Autonomic Nervous System reaches a better balance, many downstream expressions of dysregulation, including tics, often become less severe.
INSiGHT Scans
One challenge parents face is that standard medical workups, MRIs, bloodwork, and neurological exams rarely reveal what’s actually driving a child’s tic condition. That’s because conventional diagnostics look for structural problems or disease. They don’t measure function.
INSiGHT scans are a non-invasive technology that measures how well a child’s nervous system is actually functioning. These scans aren’t used to diagnose or treat any condition, not even back pain, but they do provide an objective window into the patterns of neurological dysregulation that may be contributing to a child’s struggles.
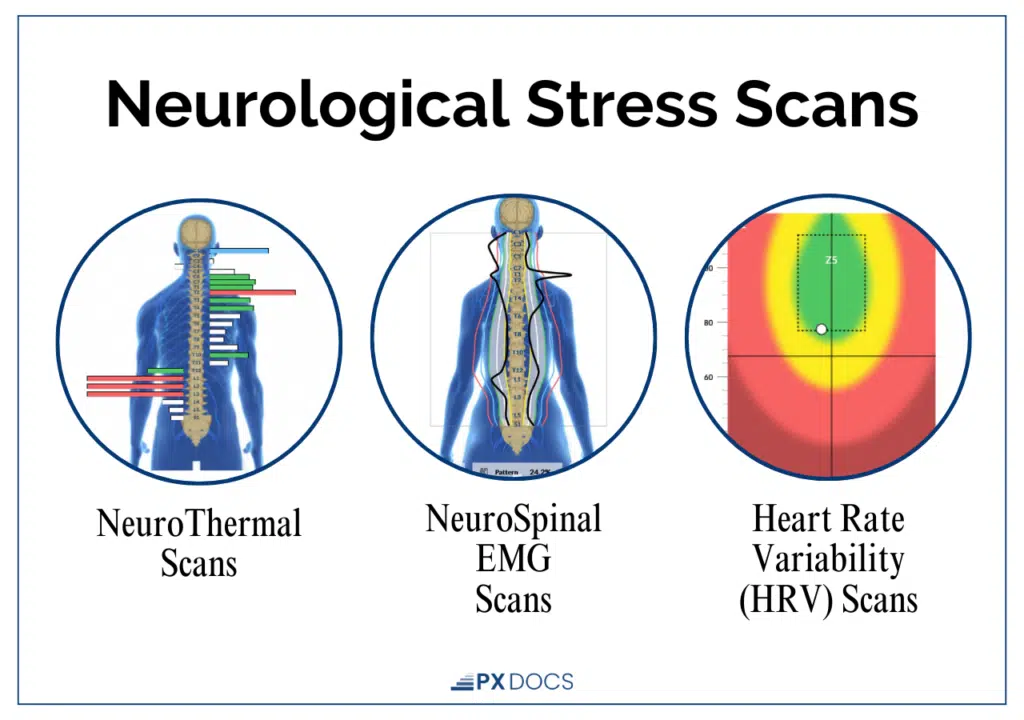
Three components make up a full INSiGHT scan:
- Heart Rate Variability (HRV): Measures the balance between the sympathetic (“fight-or-flight”) and parasympathetic (“rest, regulate, and digest”) branches of the autonomic nervous system. Lower HRV indicates the nervous system has less flexibility to adapt to stress.
- Surface Electromyography (sEMG): Assesses the electrical activity of muscles along the spine, identifying areas of neuromotor tension and altered proprioceptive function.
- Thermal Scanning: Uses infrared sensors to detect temperature asymmetries along the spine, indicating areas of dysautonomia and impaired autonomic regulation.
In children presenting with tics, these scans often reveal significant sympathetic dominance, reduced vagal tone, and patterns of neurological disorganization, exactly what the autonomic model of tic production would predict. Tracking these patterns over the course of care lets both clinicians and families see the nervous system shifting toward better regulation, often before the tics themselves visibly improve.
A More Complete Answer to What Causes Tics in Children
The conventional explanation for what causes tics in children, genetics and basal ganglia dysfunction, isn’t wrong. It’s just not the whole story.
Tics are a neurological output produced by a nervous system under more stress than it can properly regulate. The basal ganglia are the immediate mechanism, but behind them is a broader system: the Autonomic Nervous System, the vagus nerve, and the stress response pathways that were being shaped long before your child was old enough to sit in a classroom.
For many children, the foundation for tic conditions was laid early, through prenatal stress, birth trauma, early childhood neurological challenges, in what we call the “Perfect Storm.” Understanding that history doesn’t change the diagnosis. But it opens up a different set of questions, and a different set of possibilities for support.If your child is struggling with tics and you’re looking for a root-cause approach, the PX Docs directory can connect you with a Neurologically-Focused Chiropractor trained to assess these patterns and build a care plan that works from the nervous system out. That’s where real change tends to start.



