

Your child just got diagnosed with scoliosis. Or maybe the pediatrician flagged a possible curve, and you’re in that awful limbo of waiting for more tests. Either way, your first question is the obvious one: why did this happen?
Here’s what you’ll hear at most doctors’ offices: “We don’t know. In most kids, there’s no identifiable cause.” And for so many parents, that answer isn’t good enough, because it shouldn’t be.
The conventional medical explanation for scoliosis in kids covers the structural story well. It covers vertebrae, growth spurts, genetics, and X-rays. What it almost never covers is the neurological story, the role your child’s nervous system plays in controlling spinal muscle tone, maintaining postural balance, and detecting position. That’s the piece we’re going to add.
This article will walk you through everything you need to know about the causes of scoliosis in children, the signs to watch for, how it’s diagnosed, and what standard care looks like. Then we’ll show you the root-cause neurological layer that conventional medicine tends to skip, and why that matters for how you support your child’s spine long-term.
What Is Scoliosis?
Scoliosis is a sideways curvature of the spine. A healthy spine, when viewed from the back, runs straight down the center of the body. A spine with scoliosis curves to the left, right, or both, forming a “C” or “S” shape.
The vertebrae (the individual bones of the spine) don’t just tilt sideways. In most cases, they also rotate or twist, which is what creates that distinctive rib hump visible when a child bends forward.
Doctors measure scoliosis using the Cobb angle, the degree of curvature visible on X-ray. Severity is classified as:
- Mild (10–20 degrees)
- Moderate (20–40 degrees)
- Severe (40 degrees or more).
A curve needs to measure at least 10 degrees to be officially diagnosed as scoliosis.
Scoliosis is more common than most parents realize. It affects roughly 2–3% of the U.S. population, with more than 100,000 children diagnosed each year. Girls are more likely than boys to develop curves severe enough to need care. The condition is most often caught between ages 10 and 18, though it can develop at any age.
The Three Main Types of Scoliosis in Children
Understanding what causes scoliosis in kids starts with knowing that there are actually several different types, each with its own origin story.
Idiopathic Scoliosis
This is by far the most common type, accounting for more than 80% of all cases. “Idiopathic” simply means the exact cause is unknown. Children with idiopathic scoliosis don’t have an underlying disease, injury, or birth defect that explains the curve, at least not by conventional diagnostic standards.
Idiopathic scoliosis is further broken down by age at diagnosis:
- Infantile (birth to 3 years)
- Juvenile (3 to 9 years)
- Adolescent (10 to 18 years).
Adolescent Idiopathic Scoliosis (AIS) is the most common of the three and tends to worsen most rapidly during puberty growth spurts.
Genetics plays a role. According to the American Academy of Orthopaedic Surgeons, roughly 30% of children with adolescent idiopathic scoliosis have a family history of the condition, suggesting a hereditary component, though no single gene has been identified as the cause.
Congenital Scoliosis
Congenital scoliosis develops before birth when the vertebrae don’t form properly or fail to separate correctly during fetal development. Some vertebrae may be partially formed, fused together, or wedge-shaped, all of which create a structural imbalance in the spine from day one.
This is the least common type of scoliosis. It’s often part of a broader set of developmental issues and may not become obvious until a child hits a growth spurt.
Neuromuscular Scoliosis
This type develops as a secondary effect of conditions that affect the muscles or nerves, including:
- Cerebral palsy
- Muscular dystrophy
- Spina bifida
Spinal cord injuries.
When the muscles supporting the spine are too weak or unequal in strength, the spine can’t maintain a neutral position and gradually curves over time.
What Actually Causes Idiopathic Scoliosis?
Since idiopathic scoliosis represents the majority of cases, parents naturally want to know: what’s actually going on in these kids?
Here’s what the research currently supports:
- Genetics contributes significantly. Families with one affected member have a substantially higher likelihood of scoliosis in other relatives. But genetics don’t explain everything. Identical twins don’t always develop scoliosis at the same rate or severity, which tells us the environment and developmental factors matter too.
- Growth spurts are a major trigger for progression. Curves that are small and stable can accelerate rapidly when a child goes through puberty. Girls typically see the most rapid progression between ages 11 and 13; boys somewhat later. This is why kids who are still growing with moderate curves are monitored so closely; a curve can go from 20 degrees to 40 degrees within a single growth year.
- Hormonal factors have been explored, particularly since scoliosis affects girls at higher rates than boys. Research has investigated melatonin, estrogen, and growth hormone, but no definitive hormonal cause has been confirmed.
One thing the research is clear on: scoliosis is not caused by poor posture, carrying a heavy backpack, or sports activities. These are common parent concerns, and the data consistently show that they play no causal role.
Signs of Scoliosis Parents Should Watch For
Scoliosis is notoriously easy to miss, especially in the early stages. The spine curves slowly. It usually doesn’t hurt. Kids don’t feel it happening.
Here’s what to look for:
- Uneven shoulders, one sitting visibly higher than the other
- Prominent shoulder blade, one blade sticking out more than the other when standing
- Uneven hips or waist, the waistline looks higher on one side
- Head not centered over the rest of the body
- One arm appears longer than the other when the child stands straight
- A visible curve or rib hump when your child bends forward
Pain is uncommon in children with scoliosis. When it does occur, it’s more typical in larger curves or in older adolescents. Don’t wait for your child to complain of back pain before checking for a curve; most kids never will.
If you notice any of these signs, mention them at the next pediatric visit. Early detection is one of the most important factors in limiting the progression of a curve.
How Scoliosis Is Diagnosed
Diagnosis starts with the Adams Forward Bend Test, a simple, low-tech screening tool your child’s pediatrician can perform in the office. The child stands with feet together and bends forward from the waist with arms hanging free. From behind, the doctor looks for asymmetry in the ribs or spine. A rib hump or visible lateral curve in this position is a strong indicator of scoliosis.
If the Adams test raises concern, your doctor will likely refer you for X-rays. The X-ray gives a clear view of the entire spine and allows the Cobb angle to be measured precisely. A Cobb angle of 10 degrees or more, combined with vertebral rotation, confirms the diagnosis.
In some cases, especially when the curve pattern is unusual or neurological signs are present, additional imaging, such as an MRI, may be ordered to rule out other spinal conditions.
The Neurological Root Cause Most Doctors Never Discuss
Here’s where the conversation shifts.
When medicine calls scoliosis “idiopathic”, an unknown cause, it’s being honest about the limits of conventional diagnostics. X-rays show the structure. They show bone angles. What they don’t show is the neurological function that controls the muscles that hold the spine in place.
And that matters, because your child’s spine doesn’t hold itself up. It’s actively supported by a complex system of postural muscles, deep spinal muscles, paraspinal muscles, and core stabilizers, all receiving constant communication from the nervous system about where the body is in space, how much tension to maintain, and how to adapt as your child moves.
That communication is called proprioception, the body’s sense of its own position and movement. It depends on sensory receptors in the joints, muscles, and connective tissues sending accurate information to the brain, which then coordinates the appropriate muscular response.
When proprioception is functioning well, the brain continuously fine-tunes spinal muscle tone on both sides of the spine to keep it balanced. When proprioception is disrupted, when the signal going into the brain is altered, diminished, or distorted, that fine-tuning breaks down. The result is asymmetric muscle tension: tighter on one side, weaker on the other. And asymmetric muscle tension, sustained over time, can pull the spine into curves.
This is the piece that conventional medicine hasn’t fully integrated into its explanation of idiopathic scoliosis. But nervous system dysregulation affecting musculoskeletal function is increasingly recognized in the research literature, particularly for conditions that develop gradually during growth.
A 2022 systematic review and meta-analysis in the Global Spine Journal confirmed that proprioceptive deficits are consistently present in adolescent idiopathic scoliosis patients compared with healthy controls. The nervous system doesn’t just sense pain; it actively manages posture through an ongoing feedback loop. Disrupt that loop, and posture suffers.
Subluxation, Birth Trauma, and the “Perfect Storm”
So what disrupts that proprioceptive loop in children?
At PX Docs, we recognize what we call the “Perfect Storm,” a combination of early physical, chemical, and neurological stressors that can overwhelm a child’s developing nervous system, creating patterns of dysfunction that often go undetected for years.
The “Perfect Storm” frequently begins with birth trauma. The birthing process, even an uncomplicated vaginal delivery, applies significant compressive and rotational forces to a newborn’s upper neck and brainstem region. When interventions like forceps, vacuum extraction, prolonged pushing, or C-section are involved, those forces increase substantially.
And for some families, prenatal stress during pregnancy has already begun shifting the baby’s nervous system toward a heightened stress state before birth even occurs.
These stressors can create subluxation, a neurological dysfunction characterized by three simultaneous components:
- Misalignment or altered positioning within the neurospinal system
- Fixation and restricted motion in those spinal segments
- Neurological interference that disrupts sensory input to the brain.
Upper cervical subluxation, at the very top of the neck, is particularly significant for postural control. This region of the spine has an extraordinarily dense concentration of proprioceptive receptors. It’s one of the most neurologically active areas in the body. When it’s restricted and fixated, the quality of proprioceptive input going to the brainstem and brain changes. The brain receives distorted information about where the head and body are in space.
Over time, as a child grows, the nervous system compensates. Muscles on one side of the spine work harder than the other. Tension patterns develop. And if those tension patterns aren’t addressed, growth spurts, especially the dramatic ones of puberty, can accelerate them into measurable spinal curves.
None of this appears on a standard X-ray. You won’t find it in a blood panel. Conventional scoliosis diagnostics don’t assess neurological function at all; they measure what the dysfunction has already produced in bone.
How Neurologically-Focused Chiropractic Care Approaches Scoliosis
At PX Docs, Neurologically-Focused Chiropractic Care approaches scoliosis differently, not by trying to straighten the spine mechanically, but by assessing and addressing the neurological dysfunction driving muscle imbalance.
The foundation of that assessment is INSiGHT scanning technology, a non-invasive, objective way to measure nervous system function. It’s worth being clear about what these scans do and don’t do: INSiGHT scans do not diagnose, treat, or cure any condition, not even back pain, and are not designed to replace X-ray imaging. What they measure is neurological function and Autonomic Nervous System balance.
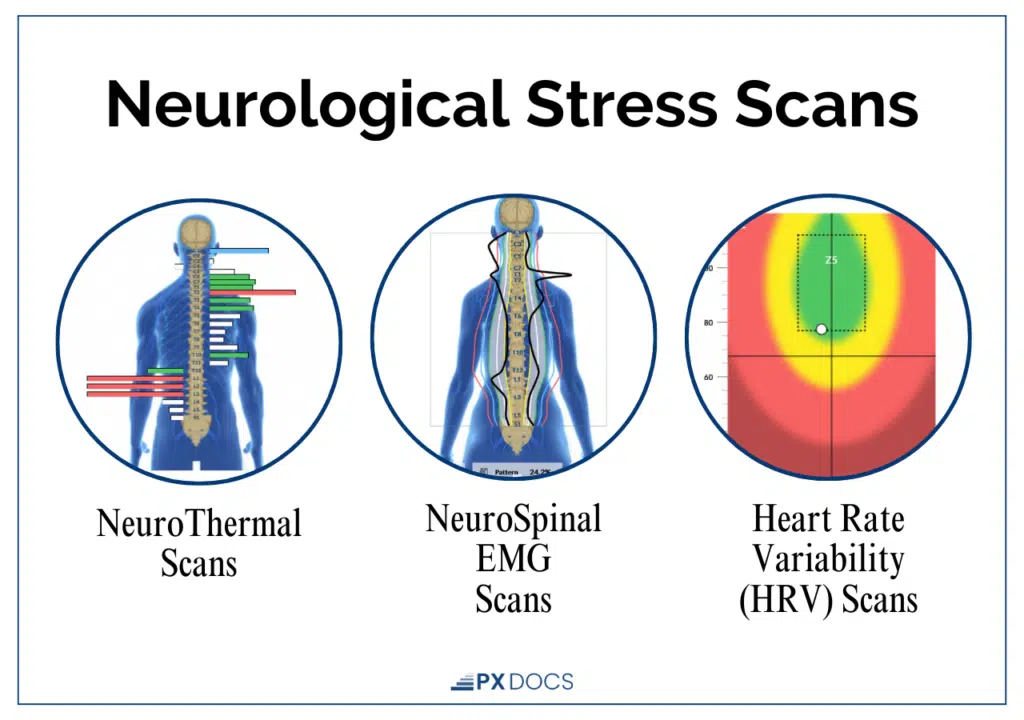
The three components of the INSiGHT scan system are directly relevant to understanding what’s happening in a child with scoliosis:
- Surface Electromyography (sEMG) assesses the electrical activity of muscles along the spine, revealing areas of tension, asymmetry, and altered neuromuscular function. In children with spinal curvatures, the sEMG often shows characteristic patterns of imbalance: muscles working too hard on one side and insufficiently engaged on the other.
- Thermal Scanning uses infrared sensors to measure temperature differences along the spine, which can indicate areas of dysautonomia, dysregulation in the autonomic nervous system that controls the blood vessels, organs, and tissues running alongside each spinal segment.
- Heart Rate Variability (HRV) measures the balance between the sympathetic (fight-or-flight) and parasympathetic (rest-and-regulate) branches of the autonomic nervous system. Children locked into sympathetic dominance, a chronically activated stress state, show poor adaptability and reduced capacity for the kind of regulated, balanced neuromuscular tone the spine depends on.
When these scans reveal patterns of neurological dysfunction, Neurologically-Focused Chiropractic Care works to address the subluxation driving it. Specific, gentle adjustments directed at restricted spinal segments restore motion and proprioceptive input. The goal isn’t to push bones into place; it’s to restore normal afferent signaling into the nervous system so the brain can do its job of coordinating balanced postural muscle tone.
This approach complements conventional scoliosis management. Parents whose children are in observation, bracing, or even preparing for surgical consultation can still benefit from addressing the neurological function that influences how the spine holds itself.
What Should You Do If Your Child Has Scoliosis?
If your child has already been diagnosed, keep your follow-up appointments. Regular X-rays are the only way to know if a curve is progressing, and that information is critical for making good decisions. If a brace has been recommended, wear it as directed. The research supporting bracing for moderate curves in growing kids is solid.
And then ask a question conventional medicine rarely raises: how is my child’s nervous system functioning?
Because a spine doesn’t curve in a vacuum. It curves as the end result of forces, structural, developmental, and neurological, working on it over time. Getting ahead of those forces, understanding what’s happening in the nervous system, and driving muscle tone and postural control are how you support your child’s spine in a way that goes beyond watching and waiting.
The nervous system is the master controller of the musculoskeletal system. That’s not a chiropractic opinion; that’s basic physiology. And it’s the piece the standard scoliosis conversation has consistently left out.
Supporting Your Child’s Spine From the Root Up
Parents dealing with a scoliosis diagnosis often feel like they’ve been handed a problem with no good answers, just a curve to watch, and hope it doesn’t get worse. That feeling is real, and it’s understandable.
You now know more than most. You understand the three types of scoliosis, how they’re diagnosed, and what the conventional care pathway looks like. You also understand why the “idiopathic” label might be less about mystery and more about what conventional diagnostics are built to see.
The nervous system controls postural muscle tone. Proprioception drives spinal balance. Subluxation from birth trauma and early life stressors can disrupt that neurological feedback loop. And that disruption, left unaddressed as a child grows, may be one of the pieces of the idiopathic puzzle.
If you want to explore whether a neurological approach could support your child’s spine health alongside conventional care, we encourage you to find a qualified Neurologically-Focused Chiropractor through the PX Docs directory. These providers are trained to assess the neurological function that standard scoliosis diagnostics don’t measure, and to work collaboratively with your child’s existing medical team.
Your child’s care deserves the whole picture.



