

Painful nursing. Endless feeds. A baby who always seems uncomfortable. If tongue or lip ties have been mentioned, chances are you’ve been told to either wait it out or head right in for the revision – but your gut knows something isn’t adding up. And you’re right.
Tongue and lip ties can make feeding and speech harder – but that’s rarely the full story. When babies also struggle with reflux, colic, constipation, or sleep, it’s a clue that the nervous system is under stress. The tie is just one piece of a bigger picture.
At PX Docs, we’ve worked with thousands of families dealing with ties, helping them look deeper than not only the associated symptoms and struggles, but deeper than even the tongue and lip ties themselves. This article will give you the complete picture of what’s going on: what ties are, how they’re cared for, and why addressing your baby’s nervous system creates lasting results beyond feeding.
What Are Tongue and Lip Ties?
A tongue tie (ankyloglossia) happens when the lingual frenulum, tissue connecting the tongue to the floor of the mouth, restricts tongue movement. An anterior tongue tie is visible when you lift your baby’s tongue. A posterior tongue tie is harder to spot because the restriction is further back.
Some babies have a thin frenulum that allows decent movement, while others have a thick band that severely limits mobility. You might notice your baby’s tongue appears heart-shaped when they cry.
A lip tie involves the labial frenulum connecting the upper lip to the gums. When this tissue is too tight, it limits lip mobility. Your baby needs to flange their upper lip outward for a good feeding seal – a lip tie prevents that. Research suggests 10% of babies have a lip or tongue tie.
While most explanations stop at describing tight tissue, the real question is why that tissue became restricted in the first place.
Common Signs Your Baby May Have Ties
Breastfeeding difficulties are the most common discovery point. Your baby might struggle to latch or can’t maintain a seal. You hear clicking sounds – that’s air getting in because the tongue can’t create a proper vacuum. Feeding sessions stretch to 45+ minutes, yet your baby still seems hungry. Poor weight gain becomes a concern. Some babies compensate by chomping instead of using proper tongue movement, creating intense nipple pain. Cracked, bleeding nipples are common. Mastitis or plugged ducts develop when milk isn’t removed efficiently.
- For bottle-fed babies: poor seal around the nipple, excessive air intake, long feeds, milk dribbling out.
- Visual signs: heart-shaped tongue when crying, can’t lift tongue to the roof of the mouth, upper lip won’t flange outward.
Here’s where the pattern gets interesting. Babies with ties often have sleep disturbances, startle easily, struggle to stay asleep, and seem uncomfortable lying flat. Many have reflux or colic. Constipation is common even in exclusively breastfed babies.
Notice how these challenges show up together – feeding, sleeping, and digestive issues. That’s not a coincidence; it’s nervous system dysregulation.
Later effects include speech difficulties (L, R, T, D, N sounds), a narrow palate leading to crowded teeth, mouth breathing, and sleep-disordered breathing. All of that can add up and contribute to Sensory Processing Disorder and even other challenges like ADHD and emotional dysregulation.
These downstream effects all trace back to nervous system dysfunction; ties are most often “middle man” signs of a deeper problem, not the root cause.
The Conventional Care Approach
A frenotomy is a quick snip, releasing tight tissue – takes seconds, works for thin tissue. A frenuloplasty is a more involved surgical lengthening for thick or complex ties. Most providers now use laser technology instead of scissors; they cauterize as they cut, which results in less bleeding.
Post-procedure exercises and adjustments are critical. The body wants to heal tissues back together. Without active use of the newly released tongue, the frenulum can reattach – sometimes tighter than before. Providers show you stretches to do several times daily for 2-4 weeks. These exercises aren’t fun (babies cry), but skipping them significantly increases the risk of reattachment.
These procedures address tissue restriction, and that matters. But tissue restriction is often a response to something deeper, which is why exercises focus on preventing reattachment, yet don’t address why the tissue was tight initially.
Why Some Babies Still Struggle After Revision
Here’s what we see regularly: a baby has their tongue tie revised, feeding improves for a few weeks, then the clicking starts again. The tongue looks restricted. The latch gets shallow. The infant stays uncomfortable and unsettled.
For parents who were told the revision would “fix everything,” this is heartbreaking – especially after fighting through all the stretches and exercises your little one couldn’t stand.
Multiple revisions aren’t uncommon; some babies need 2-4 procedures. Or feeding and sleep issues persist despite a perfect surgical technique.
Think about ear tubes. A child gets chronic infections; tubes drain fluid; infections stop. Then they come back. More tubes. The tubes address fluid accumulation, but not the reason the ears keep filling.
Tongue ties work the same way. The body creates tissue restrictions as a protective response to deeper dysfunction. When there’s neurological tension in the upper cervical spine and cranial bones, especially, the body creates compensatory patterns in surrounding tissues.
We really can’t say it enough – ties are compensatory protections, not the foundational root cause themselves.
Here’s the critical connection: neurological tone dictates soft-tissue tone. When your baby’s nervous system runs in high stress mode (sympathetic dominance), muscles throughout the body stay tense – including tiny muscles and fascial tissues around the tongue and jaw.
This explains ties that “come back” after revision. The tissue was clipped, but nervous system tension remained. The body recreated the protective restriction. It’s not surgical failure; it’s a biological response to unchanged subluxation.
The Root Cause: Your Baby’s Nervous System
Subluxation is an interference in nervous system function. In babies, this shows up as restricted movement in the upper cervical spine, cranial bones, jaw, and even other regions of the neurospinal system.
When subluxation is present, it affects the brainstem and the autonomic nervous system, which control sleep, breathing, digestion, and muscle tone. It also affects cranial nerves, particularly the vagus nerve.
This leads to dysautonomia – an autonomic nervous system imbalance.
Think of it like a car with two pedals. The sympathetic nervous system is the gas pedal, mobilizing energy, increasing heart rate, and creating muscle tension (guarding, protection). The parasympathetic and vagus nerve side is the brake pedal, which activates calming, relaxation, and regulation.
When subluxation is present, the gas pedal gets stuck on, and the brake pedal doesn’t work – so the child’s entire body stays in “fight or flight” protection mode, including the tiny muscles around the tongue, lips, and jaw.
What Triggers This “Perfect Storm”
Why do some babies have ties while others don’t? It’s about accumulated stress during critical developmental periods—the “Perfect Storm.”
- Prenatal stress: High maternal stress during pregnancy means cortisol and stress hormones cross the placenta, altering how the baby’s nervous system develops.
- Birth trauma: Interventions like forceps, vacuum extraction, C-section, induction or prolonged labor apply forces to the baby’s head and neck. The upper cervical spine and cranial bones, in particular, are incredibly delicate at birth. When physical forces compress or interfere with these structures, subluxation occurs.
- Early stressors and toxic overload: Babies with nervous system dysfunction often develop colic, reflux, constipation, frequent infections, all signs of dysautonomia. Antibiotics further disrupt gut microbiome and vagus nerve function.
The Vagus Nerve Connection
The vagus nerve exits the skull through the jugular foramen, right where the temporal bone meets the occipital bone at the skull base. This nerve controls tongue movement, jaw coordination, swallowing reflexes, digestion, heart rate, emotional regulation, and immune function.
During birth interventions, these cranial bones can be compressed or disrupted, affecting vagus nerve function right where it exits.
When your baby can’t coordinate their tongue for feeding, it’s not primarily a tongue problem – it’s a vagus nerve problem. It’s a neurological problem more than a soft-tissue issue.
The same nerve controlling tongue movement also controls digestion, sensory processing, and emotional regulation – which is the real connection to various “Perfect Storm” struggles and conditions later in life that have been connected to tongue and lip ties, airway issues, etc.
This is why your baby with a tongue tie also has reflux, colic, and can’t sleep. It’s not four separate problems; it’s one nervous system stuck in stress mode showing up in four ways.
A Different Approach: Addressing the Foundation First
Neurologically-Focused Chiropractic Care focuses on finding and gently addressing areas of tension and stress within the cranial, upper cervical, and neurospinal system. By reducing interference in the nervous system, we help your baby’s body relax, reconnect, and function the way it was designed to.
These super safe adjustments activate the vagus nerve and help shift the nervous system from sympathetic dominance into parasympathetic regulation.
Neurological INSiGHT Scans: Finding Subluxation & Dysfunction
INSiGHT Scans look far deeper than any physical examination can, detecting the presence of subluxation, dysfunction, and dysautonomia as early as a few days old in little ones. They are non-invasive and take less than 15 minutes, giving parents the root cause answers they’ve been searching for.
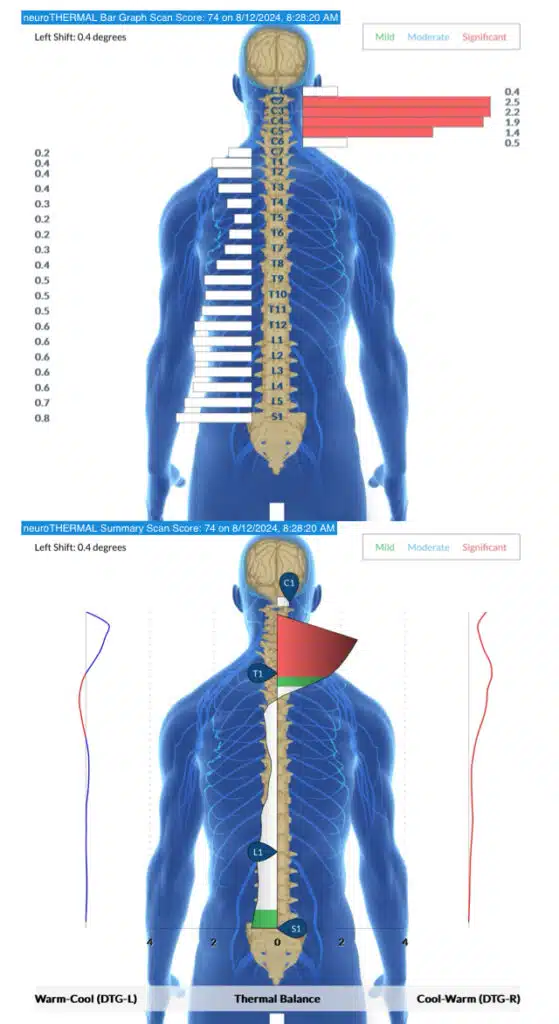
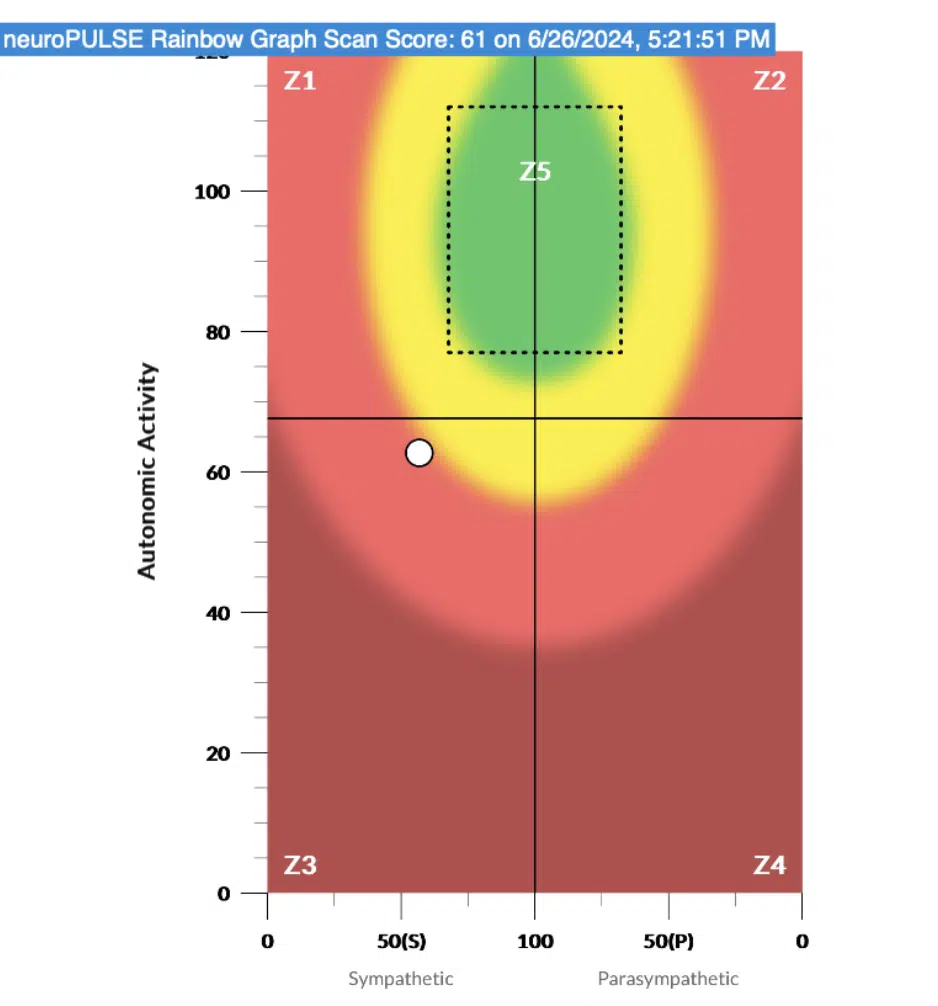
Below is an example of an INSiGHT Thermal and HRV (Heart Rate Variability) scan, indicating the presence of subluxation in the upper cervical (C1 + C2) region, most commonly associated with tongue and lip ties, as well as full neurological exhaustion (seen on HRV), commonly associated with sleep difficulties and tension stuck deep within the system.
Common Clinical Outcomes
When nervous system dysfunction is addressed first, many things improve simultaneously. Some ties resolve with adjustments alone – facial tension releases, tongue moves more freely, and feeding improves without revision.
Other times, addressing the nervous system first makes revision more successful if needed, especially when it comes to optimal recovery and lasting results. The body isn’t working against the release. Reattachment is less likely.
But here’s what really matters: sleep improves, digestion regulates, temperament calms. These are all signs of a nervous system shifting out of sympathetic dominance into a balanced, regulated state.
[INSERT TONGUE TIE + COLIC CONNECTED TESTIMONIAL]
When Revision IS the Right Choice
We’re not anti-revision. Some ties are severe enough that tissue release is necessary. The key is timing and sequence: address the nervous system first, then assess whether revision is still needed. If revision proceeds, ongoing nervous system care helps prevent recurrence and supports optimal healing.
Supporting Your Baby at Home
Skin-to-skin contact provides co-regulation; your calm nervous system helps regulate your baby’s. Biological nurturing feeding positions (laid-back, baby on your chest) reduce stress on the neck and jaw. Avoid sleep training with prolonged crying in the first year; crying activates the sympathetic nervous system.
The Bottom Line
Tongue and lip ties can absolutely impact feeding and early development, and addressing the physical restriction often helps. But when challenges linger, return, or show up alongside things like reflux, tension, poor sleep, or difficulty calming, it’s often a sign that the nervous system itself needs support.
Tight tissue is rarely the whole story – it’s usually the body communicating a deeper level of distress on the nervous system itself. That’s why it’s important to work with providers who look at the whole picture, not just the mouth.
Practitioners trained in Neurologically Focused Pediatric Care use gentle assessments, objective scans, and specific infant techniques to understand how your baby’s nervous system is functioning and how to best support it. You can explore the PX Docs directory to find a Neurologically-Focused Pediatric Chiropractor near you.
When the nervous system is supported, and stress patterns are reduced, babies can relax, regulate, and thrive – not just with feeding, but with sleep, digestion, comfort, and development. Trust your instincts. If something doesn’t feel right, that matters. There is real hope when care addresses what’s happening beneath the surface.



