

It’s the moment every parent dreads. You’re at the grocery store when suddenly your child erupts into a screaming, flailing episode on the floor. Or maybe it’s 3:15 p.m. and your kid, described all day as an angel by the teacher, falls apart the second they buckle into the car. All you can hear in that cacophony of wails and judgmental stares is the sound of parental defeat.
If this sounds painfully familiar, know that you are far from alone. According to the CDC, approximately 1 in 6 children in the United States has a developmental challenge, which can manifest as behavioral challenges, including meltdowns and sensory issues. While they look similar, meltdowns and tantrums have different origins and demand distinct approaches. And one specific pattern, what experts now call after-school restraint collapse, deserves its own conversation, because it’s one of the most common reasons parents reach out to our offices.
We’re going to clarify those key meltdown vs tantrum differences, helping you identify whether an outburst stems from behavioral or neurological causes. You’ll also learn what after-school restraint collapse looks like, why some children are far more prone to it than others, and practical strategies for both—all through a unique lens: the nervous system’s role in childhood emotional regulation.
Tantrums: Outbursts of Unmet Desires
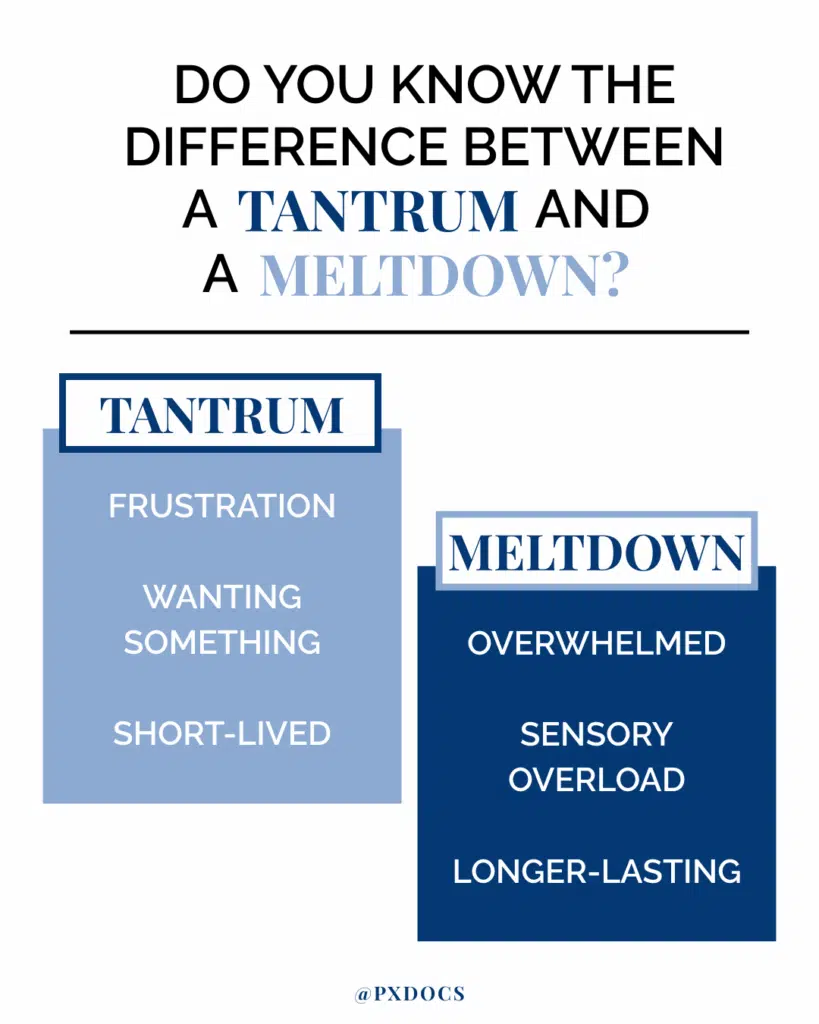
During a tantrum, a child may throw themselves to the ground, kick, scream, and flail in an unabashedly demonstrative display of emotion. While undeniably unpleasant, tantrums are part of typical childhood development, typically beginning around 18 months and peaking between ages 2-3 as children develop language and emotional regulation abilities. During this stage, kids lack the vocabulary to express complex feelings and the self-control to manage frustration appropriately.
At their core, tantrums are behavioral outbursts that erupt when a child’s immediate want or perceived need goes unfulfilled. Some of the most common tantrum triggers include:
- Wanting a toy or treat at the store
- Not wanting to leave a fun place or activity
- Feeling frustrated with a challenging task
- Resisting a daily routine like bedtime or tooth brushing
In the moment, a tantrum is a tactic a child uses to get their way. These attention-seeking behaviors may involve testing limits, seeking reactions, or attempting to manipulate situations. As unpleasant as they are, tantrums serve a developmental purpose in helping children learn about the balance between their desires and the necessary boundaries in life.
Meltdowns: Neurological Crises of Sensory Overload
While they may look similar on the surface, there’s a big difference between a tantrum and a meltdown. Meltdowns are a fundamentally different experience for a child. If a tantrum is a behavioral choice to act out, a meltdown is a neurological event marked by complete loss of control.
During a meltdown, such as in the case of an autism meltdown or with Sensory Processing Disorder, the child has reached a point of such intense sensory and emotional overload that their brain effectively short-circuits and can no longer process information or cope with surrounding demands.
This neurological shutdown triggers the fight-or-flight response, activating the Autonomic Nervous System’s survival mode. During this autonomic response, the prefrontal cortex, responsible for rational thought and emotional regulation, goes offline. This is why reasoning with a child in meltdown mode is futile. Their brains have shifted entirely into survival mode, focused solely on escaping the overwhelming stimuli.
In these moments, the child often feels overwhelmed, flooded with inexplicable emotion, and unable to articulate their distress. Some may even experience dissociation, feeling disconnected from their body and surroundings.
What Does a Meltdown Feel Like From Inside?
Understanding the internal experience of a meltdown helps us respond with empathy rather than frustration. Research from a study with 32 adults with autism described what meltdowns feel like from the inside: being overwhelmed by sensory, cognitive, or social triggers; feeling intense fear or anger; losing cognitive clarity; dissociation; and emotional release that may include self-harm. Many described experiencing “internal meltdowns” that weren’t visible to others but were just as distressing.
For children experiencing meltdowns, the world becomes too much: sounds are unbearably loud, lights are painfully bright, textures are overwhelmingly intense. Their nervous system floods with stress signals, creating a cascade of physiological dysregulation they cannot control or stop through willpower alone.
Notably, typical behavior strategies cannot resolve meltdowns in the moment. Reasoning with a child in meltdown mode is futile because their cognitive capacities are offline. Ignoring the episode or making demands will only heighten their distress. Even giving in to any initial request that may have preceded the meltdown will not calm them, as the root issue is not a desire for control but a loss of regulatory control.
Another key distinction is that while tantrums are most common in toddlers and preschoolers, meltdowns can occur at any age. This is especially true for individuals with neurological differences or sensory processing sensitivities. Neurodivergent individuals—including those with Autism Spectrum Disorder, ADHD, or other neurodevelopmental differences—may continue experiencing meltdowns throughout their lives as their nervous systems remain more susceptible to sensory overload.
Exploring the Key Difference Between a Tantrum vs Meltdown
Despite their outward similarities, tantrums and meltdowns differ considerably in their triggers, onset, resolution, and neurological basis. Distinguishing between the two is the first step in forming an appropriate action plan to help your child through either scenario.
Triggers
Tantrums are typically triggered by a single unmet want or need, such as not getting a desired toy or treat. Meltdowns, on the other hand, result from cumulative overstimulation or a perceived threat that pushes the nervous system past its coping threshold. Common sensory overload triggers include:
- Loud noises
- Bright lights
- Crowded spaces
- Competing sounds
- Scratchy clothing
- Unexpected changes in routine
Onset
Tantrums often occur quickly and intensely when the child’s desire is thwarted. In contrast, meltdowns tend to build gradually, with the child exhibiting subtle cues of growing dysregulation before reaching a point of no return.
Warning signs may include:
- Avoidance of eye contact or interaction
- Covering ears or eyes
- Increased fidgeting or pacing
- Verbal protests of distress
- Bolting or eloping from an activity
Outward Signs
During a tantrum, a child will continue to make demands and express what they want. Conversely, a meltdown involves less clear verbal communication, with reactions such as screaming, shrieking, or total withdrawal being more prominent fight-flight-freeze responses.
Audience Dependency
Tantrums almost always require an audience, someone who can potentially grant the child’s wish. Children rarely tantrum when alone. Meltdowns, conversely, occur regardless of who’s present and may happen more frequently in new environments or with unfamiliar people, as these situations create additional sensory overload.
Resolution
Most tantrums can be resolved relatively quickly, either by granting the original request, creating a distraction, or outlasting the outburst. Meltdowns, however, cannot be truncated by reasoning and require time for the nervous system to regulate again. They often last 20 minutes or longer, even after the stimulus is removed.
Recovery Patterns
After a tantrum ends, children typically recover quickly and can resume activities normally. Following a meltdown, however, children need significant recovery time. They may appear exhausted, confused, or emotionally drained, a physiological response to the intense activation of their nervous systems.
How Do I Know If It’s a Tantrum or Meltdown?
When your child is in the midst of an intense episode, distinguishing between a tantrum and a meltdown isn’t always straightforward. However, a few key observations can help you identify what’s actually happening—and respond appropriately.
Ask yourself these questions:
- The Audience Test: Does the behavior change when you leave the room or stop watching? If yes → likely tantrum. If the episode continues or intensifies regardless of your attention → likely meltdown.
- The Resolution Test: Does giving in to the request stop the behavior immediately? If yes → tantrum. If the behavior continues even after the original trigger is addressed → likely meltdown.
- The Warning Signs Test: Did the episode start suddenly after hearing ‘no,’ or did you notice building signs like covering ears, increased movement, or withdrawal? Sudden onset → tantrum. Gradual escalation with warning signs → meltdown.
- The Recovery Test: Once the episode ends, does your child bounce back quickly, or do they seem exhausted and need quiet time? Quick recovery → tantrum. Extended recovery time → meltdown.
What Is After-School Restraint Collapse?
There’s one specific pattern that fits all four meltdown criteria above—and it has a name. After-school restraint collapse is what happens when a child holds it together all day at school, then falls apart the moment they reach the safety of home or the car at pickup. The term was coined by Canadian counselor and parenting educator Andrea Loewen Nair, and it describes a phenomenon nearly every parent of a school-aged child has witnessed.
Here’s the dynamic: during the school day, your child uses enormous cognitive and emotional energy to follow rules, sit still, manage transitions, process noise and lights, navigate friendships, and regulate big feelings. That self-control isn’t free—it draws from a finite regulatory reserve. By the time the bell rings, the tank is empty. Home is the one place safe enough to let the guard down. So they do. Often dramatically.
Signs of after-school restraint collapse include:
- Sudden tears or angry outbursts within minutes of pickup
- Wild, silly, hyperactive behavior that escalates instead of settling
- Refusing to talk about the school day or shutting down completely
- Lashing out at parents or siblings over minor requests
- Extreme fatigue, hunger, or thirst that wasn’t addressed at school
- Crying that feels disproportionate to anything that just happened
After-school restraint collapse isn’t a diagnosis. It’s a predictable pattern that’s widely recognized by educators, pediatric clinicians, and therapists, and it shows up most intensely in children whose nervous systems are already running closer to overload. That includes kids with sensory processing differences, ADHD, anxiety, autism, school refusal patterns, or any condition that makes the school environment feel more demanding than it does for their peers.
Is After-School Restraint Collapse a Tantrum or a Meltdown?
Run it through the four tests above, and the answer is clear. After-school restraint collapse almost always behaves like a meltdown: it doesn’t stop when you leave the room; giving in to a request doesn’t end it; warning signs were building all day, even if you couldn’t see them; and recovery takes real time. The trigger that finally tips your child over—being asked to take off their shoes, or a sibling looking at them sideways—isn’t the cause. It’s the last straw on a nervous system that’s been carrying weight all day.
That distinction matters because it changes how you respond. Punishing a meltdown for a “small” trigger only adds stress to a system that’s already maxed out.
Meltdown vs Tantrum: “The Perfect Storm” of Neurological Origins and Differences
While tantrums originate as reactions to unmet desires, meltdowns run much deeper, reflecting nervous system imbalances related to a phenomenon we call “The Perfect Storm.” This concept acknowledges that accumulated stressors very early in life can impact the developing nervous system, leaving children more vulnerable to meltdown episodes later. It’s also the reason some kids handle the school day with energy to spare while others arrive home in pieces.
“The Perfect Storm” sequence usually involves:
- Prenatal stress exposure: Maternal anxiety or trauma during pregnancy can affect the baby’s nervous system, making it harder for the baby to regulate intense arousal after birth.
- Birth interventions and subluxation: Procedures like C-sections, forceps deliveries, and vacuum extractions introduce significant stress to the baby’s nervous system during a critical time for brain wiring. This can lead to subluxation—a neurological dysfunction with three components: misalignment within the neurospinal system, fixation or restricted motion in those segments, and the neurological interference that follows when brain-body communication gets disrupted.
- Ongoing sympathetic dominance: With the nervous system already taxed and subluxation limiting vagal nerve activity, the child gets stuck in a neurological “fight-or-flight” loop. This nervous system dysregulation feeds the meltdown cycle.
This ongoing Autonomic Nervous System imbalance creates a state where children exist in constant low-level stress. Their nervous system operates with a hair-trigger response to any additional stressors—their “gas pedal” stuck down, their “brake pedal” not working. What looks like ‘overreacting’ to small triggers is actually the final straw for a nervous system already operating at maximum capacity.
This is also why after-school restraint collapse hits some kids so much harder than others. A child whose Autonomic Nervous System is already running in high gear has very little reserve left to manage a six- or seven-hour school day. The school environment isn’t doing anything unusual—it’s just exposing a regulatory limit that was already there. Kids with well-regulated nervous systems absorb the same demands and arrive home with capacity to spare. The difference isn’t willpower or parenting. It’s wiring.
In essence, meltdowns are cries of distress from an overwhelmed nervous system, not acts of willful defiance. Punishments fuel further imbalance, causing the brain to perceive parental responses as threatening. The solution, therefore, lies in supporting children’s resiliency and adaptability to circumstances from the inside out, not just imposing order from the outside in.
Recognizing Warning Signs and Preventing Meltdowns
Since meltdowns represent neurological overload, the first step in preventing or mitigating them is learning to recognize your child’s unique distress signals. These cues indicate your child’s nervous system is becoming overstimulated and needs coping support before reaching critical mass.
Physical signs may include:
- Sweaty palms
- Flushed cheeks
- Rapid, shallow breathing
- Restless movements or freezing up
Behavioral shifts like these also indicate rising panic:
- Covering eyes or ears
- Bolting from activities
- Louder vocalizations
- Less responsiveness to instructions
Essentially, the earlier you spot brewing dysregulation, the more quickly you can intervene with calming input to avert complete meltdowns. Subtle redirection, movement breaks, or sensory supports given before the point of no return help your child regain equilibrium more readily.
How Can I Prevent Meltdowns?
Preventing meltdowns begins with managing sensory overload in your child’s environment. Consider reducing visual clutter in main living spaces, using softer lighting or dimmer switches, establishing quiet zones where your child can retreat when overwhelmed, minimizing competing noises (TV + conversation + running appliances), and maintaining consistent daily routines to reduce cognitive load.
Practical prevention also includes: ensuring adequate sleep and nutrition (physiological dysregulation can trigger meltdowns), teaching age-appropriate coping strategies during calm moments, creating visual schedules for transitions, using a ‘calm-down corner’ with sensory tools like weighted blankets and noise-canceling headphones, and learning your child’s unique warning signs to intervene early.
Specifically, for after-school restraint collapse, the pickup window itself matters. Try meeting basic biological needs first—a protein snack, water, a bathroom break—before any conversation or expectation. Skip the “how was school?” interrogation; it asks the most depleted part of the brain to do more work. Build in 20 to 30 minutes of low-demand decompression: quiet play, time outside, or movement-based release like jumping on a trampoline. These small adjustments can dramatically reduce the daily collapse pattern.
Beyond environmental changes, the most effective meltdown prevention addresses the root cause: nervous system dysregulation. When your child’s nervous system operates in a balanced state rather than stuck in sympathetic dominance, their capacity to handle daily stressors increases dramatically.
This is where Neurologically-Focused Chiropractic Care becomes preventive rather than reactive, using advanced INSiGHT scanning technology to identify patterns of nervous system stress and address underlying imbalances before they manifest as frequent meltdowns or daily restraint collapse.
How to Help During a Meltdown
Understanding why specific approaches work during meltdowns helps you implement them more effectively. Your child’s Autonomic Nervous System is in survival mode—the fight-or-flight response has taken over. Your goal isn’t to teach or reason, but to help their nervous system shift back to a regulated state through external calming techniques and co-regulation.
When a meltdown occurs, remember that your goal isn’t to stifle the storm of emotions but to anchor your child with your calming presence as it passes. You can’t logic or lecture them out of a meltdown, but you can ride out the wave alongside them with these steps:
- Ensure safety: If your child is at risk of harming themselves or others, quickly guide them to a less hazardous setting and remove any dangerous objects. You may need to provide a physical boundary around them using furniture or your own body to prevent bolting or head-banging, but avoid restraining unless necessary for protection.
- Stay regulated yourself: Take a slow, deep breath and adopt a soft, neutral facial expression and tone of voice. Your nonverbal cues communicate safety to your child’s nervous system. It will only heighten their distress if you seem panicked, angry, or emotionally volatile. Channel your calm to help co-regulate their emotions.
- Validate their distress: Let your child know that you’re there with them and that these intense feelings, while scary, are temporary and not “bad.” You might say, “I see you’re having a hard time. I’m here,” or “It’s okay to feel this way. You’re safe, and we’ll get through it together.” If words agitate your child, simply sit quietly nearby.
- Reduce environmental stimuli: Dim bright lights, turn off music or screens, and encourage others to move away and reduce noise. The more you can minimize sensory input, the more capacity your child will have to regain their regulatory footing. Guide them to a quiet space or other pre-established “meltdown zone” if they’re open to moving.
- Offer regulating supports: After the peak of the meltdown, your child may be receptive to calming strategies. Try these depending on their preferences:
- Sips of cold water or crunchy snacks
- Rhythmic, regulating sounds or music
- Deep pressure input (bear hugs, squeezes, weighted blankets)
- Deep breathing exercises (“Smell the flower, blow the pinwheel”)
- Visual imagery (glitter jars, guided relaxation script)
A Different Approach: Neurologically-Focused Chiropractic Care
While the responsive strategies above are helpful, one approach focuses on addressing the root cause: nervous system imbalances that make it hard for children to regulate stress. This is where Neurologically-Focused Chiropractic Care offers immense hope—especially for children stuck in repeating cycles of meltdowns, tantrums, or after-school restraint collapse.
It’s important to note that INSiGHT scanning technology does not diagnose medical conditions, and Neurologically-Focused Chiropractic Care is not a cure for meltdowns, tantrums, autism, sensory processing differences, ADHD, or any other condition, not even back pain. INSiGHT Scans help us track down the root cause of nervous system dysfunction and dysregulation, then build customized care plans and adjust protocols to help shift the nervous system back into balance, regulation, and resilience.
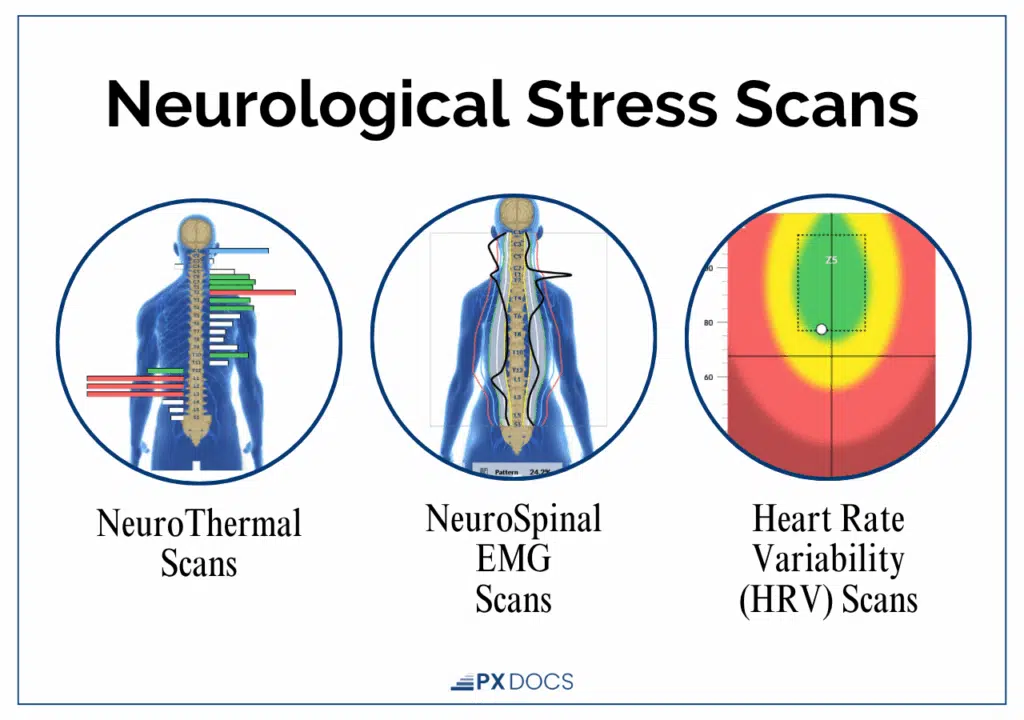
Unlike conventional pediatric care, which focuses more on trait suppression, Neurologically-Focused Chiropractors recognize how neurophysiological misalignments can alter nervous system function and perpetuate chronic stress responses. Using specialized assessments like INSiGHT Scans, they identify areas of dysregulation and develop strategic care plans to help children build the regulatory capacity their school days demand. The goal isn’t better behavior. It’s giving the nervous system more room to handle the load.
If you suspect your child’s meltdowns—or daily after-school restraint collapse—are rooted in nervous system imbalances or the lingering effects of “The Perfect Storm,” visit our PX Docs Directory to connect with a provider near you. A calmer, more resilient foundation for your whole family is possible, and it starts with aligning the brain and body for balance.



