

Tactile defensiveness is a neurological condition in which the brain interprets ordinary touch sensations, such as clothing textures, light physical contact, food textures, and grooming, as threatening or painful. It is a form of sensory over-responsivity rooted in Autonomic Nervous System dysfunction, and population-based research estimates it affects up to 13% of school-aged children. Tactile defensiveness is closely associated with Sensory Processing Disorder, Autism Spectrum Disorder, and ADHD.
If your child screams when you brush their hair, refuses to wear socks with seams, melts down over clothing tags, or avoids messy play like it’s physically painful, you’re not dealing with a “behavioral problem.”
Here’s what most articles about tactile defensiveness won’t tell you: this isn’t just a “sensory quirk.” Tactile defensiveness is a sign that your child’s nervous system is stuck in a protective, fight-or-flight state, and their brain is interpreting safe, everyday touch as a genuine threat. Understanding why that’s happening changes everything about how you approach it.
What Is Tactile Defensiveness?
Tactile defensiveness is a heightened, negative reaction to touch sensations that most people experience as neutral or harmless. First described by occupational therapist Dr. A. Jean Ayres, it occurs when the brain misinterprets ordinary tactile input—such as clothing textures, light touch, hugs, and food textures—as dangerous or painful.
Occupational therapists also refer to this as tactile hypersensitivity, tactile over-responsivity, or touch sensitivity. The terms are interchangeable, but they all describe the same underlying problem: the nervous system’s threat-detection system is dialed way too high.
For a child with tactile defensiveness, a clothing tag doesn’t just feel annoying; it feels like something is wrong. A light touch on the arm doesn’t feel casual; it triggers the same alarm response you’d have if something hot touched your skin. Their brain’s protective system activates, and they respond with fight (hitting, pushing), flight (pulling away, running), or freeze (shutting down, going rigid).
This is a neurological response.
What Are the Signs of Tactile Defensiveness in Children?
Tactile defensiveness shows up differently from child to child, but parents typically notice patterns across several areas of daily life.
Common signs of tactile defensiveness in children include:
- Distress over clothing textures, tags, seams, or waistbands
- Refusing to wear socks, shoes, or certain fabrics
- Avoiding messy textures like finger paint, glue, sand, or playdough
- Strong reactions to having hair brushed, teeth brushed, nails trimmed, or face washed
- Pulling away from light touch or unexpected physical contact
- Preference for self-initiated touch over being touched by others
- Difficulty tolerating hugs, kisses, or casual physical affection
- Food texture aversions, avoiding crunchy, mushy, or mixed-texture foods
- Resistance to walking barefoot on grass, sand, or carpet
- Meltdowns at haircuts or medical appointments involving touch
- Difficulty standing in line or sitting close to other children
These reactions often get labeled as “behavioral problems,” “pickiness,” or “overreacting.” But research from the Collaborative on the Clinical Assessment of Sensory Issues confirms these are nervous system-driven responses, not willful defiance. Children with tactile defensiveness aren’t choosing to be difficult; their nervous system is genuinely perceiving everyday touch as a threat.
Stress, fatigue, illness, and anxiety often make these reactions worse. A child who tolerates a certain shirt on Monday might completely fall apart over it on Wednesday, and that inconsistency is itself a hallmark of nervous system dysregulation.
What Causes Tactile Defensiveness?
Tactile defensiveness is caused by dysfunction in the Autonomic Nervous System, the part of your child’s nervous system that operates below conscious control, managing functions such as heart rate, digestion, sleep, immune function, and how the brain processes sensory input. When this system is dysregulated, the brain’s threat-detection filters are set too high, and ordinary touch gets flagged as dangerous.
The Autonomic Nervous System has two main branches. Think of it like a car with a gas pedal and a brake pedal.
- The Sympathetic Nervous System is the gas pedal: it accelerates the body into fight-or-flight mode when there’s a perceived threat.
- The Parasympathetic Nervous System is the brake pedal: it calms the body down, supports digestion, sleep, immune function, and helps the brain process sensory input accurately.
In children with tactile defensiveness, the gas pedal is stuck on. Their Sympathetic Nervous System is chronically overactivated, a state called sympathetic dominance, and their parasympathetic brake pedal, driven largely by the vagus nerve, isn’t providing enough calming input to balance things out.
A 2010 study found that children with sensory modulation difficulties had significantly lower baseline vagal tone than typically developing children, indicating their parasympathetic “brake pedal” was underperforming. This lower vagal tone was present across nearly all sensory challenges tested, including tactile, auditory, visual, and vestibular.
This is why tactile defensiveness rarely shows up alone. Children who are hypersensitive to touch often also struggle with sound sensitivity, difficulty with transitions, sleep disruptions, digestive issues, and emotional meltdowns. It’s the same underlying nervous system dysregulation showing up across multiple systems.
Is Tactile Defensiveness Connected to Autism and ADHD?
Children with tactile defensiveness frequently also experience autism, ADHD, anxiety, and other neurodevelopmental challenges. This co-occurrence is not coincidental; these conditions share the same underlying mechanism of Autonomic Nervous System dysfunction and dysautonomia.
Tactile symptoms are among the most commonly reported sensory symptoms in children with Autism Spectrum Disorder. A population-based twin study found that tactile defensiveness was modestly associated with fearful temperament and anxiety, with evidence of genetic influence on sensory defensiveness patterns.
Research has also found sex differences in tactile defensiveness among children with ADHD, with girls with ADHD displaying higher levels of touch sensitivity than boys with ADHD.
What this tells us is that tactile defensiveness isn’t a standalone issue. It’s often one visible expression of a deeper pattern of nervous system dysregulation that simultaneously affects sensory processing, emotional regulation, immune function, gut health, and motor development.
When you only address the tactile defensiveness without looking at what’s driving it neurologically, you’re working on one branch of the tree rather than the roots.
How Does “The Perfect Storm” Lead to Tactile Defensiveness?
At PX Docs, we’ve seen thousands of children with tactile defensiveness, and the pattern is remarkably consistent. The nervous system dysfunction driving their touch sensitivity didn’t start the day the signs appeared; it typically traces back to what we call “The Perfect Storm.”
“The Perfect Storm” describes a sequence of early-life stressors that compound on each other during the most critical periods of nervous system development:
- Stage 1: Prenatal Stress and Maternal Health. Chronic stress during pregnancy elevates cortisol levels that cross the placenta and directly affect the developing fetal nervous system. Fertility challenges, medication use, and high-stress pregnancies set the stage before a child is ever born.
- Stage 2: Birth Trauma and Interventions. Complications during labor and delivery—prolonged labor, fetal distress, forceps, vacuum extraction, induction, and C-section delivery—can create physical stress to the infant’s brainstem and upper cervical spine. This area is ground zero for Autonomic Nervous System function, and birth trauma to this region can disrupt the neurological wiring that controls how the brain processes all sensory input, including touch.
- Stage 3: Early Childhood Stressors. After birth, environmental toxins, frequent antibiotic use, chronic illness, and accumulated stress continue to load an already-compromised nervous system. The body stays stuck in sympathetic fight-or-flight mode, and the child’s ability to accurately process touch information gets progressively more disrupted.
When this cascade of stressors overwhelms the developing nervous system, it can lead to subluxation, a neurological dysfunction characterized by misalignment, fixation, and neurological interference within the neurospinal system. Subluxation disrupts the normal flow of proprioceptive and sensory input to the brain, and this disrupted input is directly connected to how a child experiences touch.
In children, subluxation commonly presents as altered sensory input, sensory overload, and disrupted sensory-motor coordination, which is exactly what we see in tactile defensiveness.
Why Doesn’t Occupational Therapy Always Resolve Tactile Defensiveness?
Let’s be clear, occupational therapy is valuable. OTs who specialize in sensory integration do important work helping children build tolerance to different textures and tactile experiences. We respect and encourage families to work with skilled occupational therapists.
But here’s what many parents discover: their child makes progress in OT sessions, but the improvements don’t always hold. The sensory challenges keep cycling back. Good days and bad days seem random. Progress is slow, and sometimes it stalls completely.
This often happens because occupational therapy works primarily at the level of the brain’s learned responses, teaching the brain to interpret touch differently through repeated exposure and sensory activities. That’s important work. But if the Autonomic Nervous System is still stuck in a chronic fight-or-flight state, the brain keeps defaulting to its threat-detection mode no matter how many sensory bins and brushing protocols you try.
It’s like trying to teach someone to relax while they’re standing on a fire; the input from below keeps overriding the learning from above.
This is why many families find the greatest progress when they combine occupational therapy with care that directly addresses the nervous system dysfunction driving the sensory overload in the first place.
How Does Neurologically-Focused Chiropractic Care Address Tactile Defensiveness?
It’s important to note that INSiGHT Scanning technology does not diagnose medical conditions, and Neurologically-Focused Chiropractic Care is certainly not a treatment or cure for tactile defensiveness or any other condition, not even back pain. Instead, these INSiGHT Scans help us track down the root cause of nervous system dysfunction and dysregulation, and build customized care plans and adjusting protocols to help shift the nervous system back into a state of balance, regulation, and resilience.
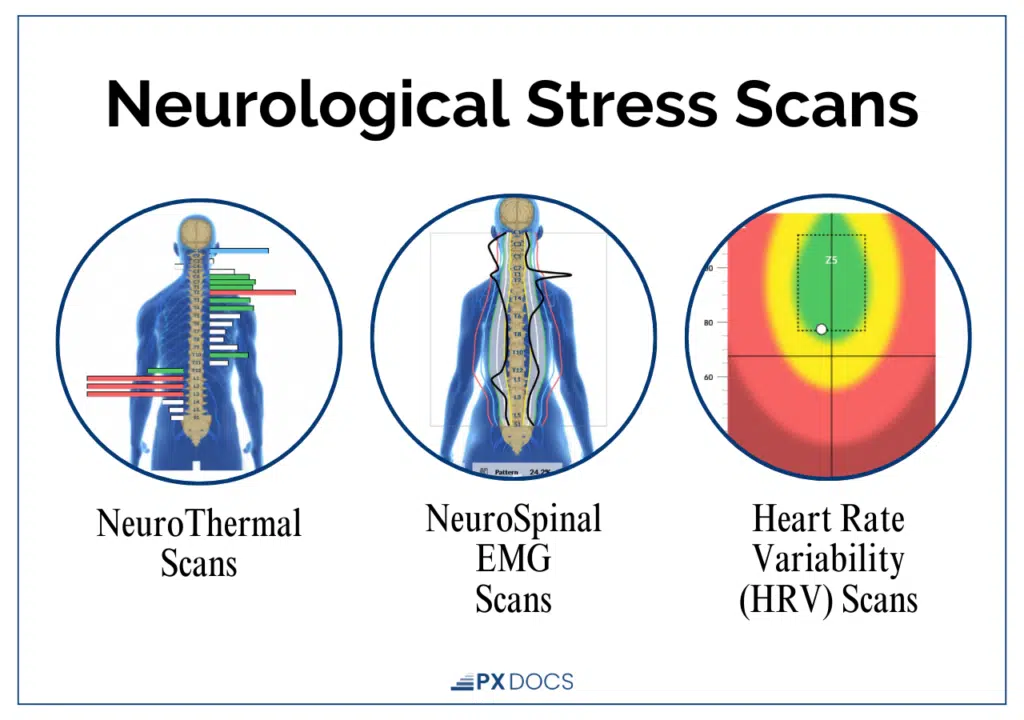
This technology includes three components:
- Heart Rate Variability (HRV) Analysis measures the balance between the Sympathetic Nervous System (fight-or-flight) and Parasympathetic Nervous System (rest, regulate, and digest) branches of the Autonomic Nervous System. For children with tactile defensiveness, HRV scans frequently show significant sympathetic dominance, the “gas pedal” stuck on.
- Surface Electromyography (sEMG) assesses the electrical activity of muscles along the spine, helping to identify areas of tension and altered neuromuscular function or proprioception. In tactile-defensive children, sEMG patterns often reveal excessive neuromotor tension, especially in the upper cervical and brainstem regions.
- Thermal Scanning uses infrared sensors to measure temperature differences along the spine, which can indicate areas of dysautonomia and autonomic imbalance.
What makes these scans valuable is their ability to detect subtle changes in neurological function long before those changes show up as symptom improvements. When a child’s nervous system begins to shift out of sympathetic dominance, the scans capture it—even before the child starts tolerating socks or letting you brush their hair without a meltdown.
When INSiGHT scans identify patterns of subluxation and nervous system dysfunction, PX Docs practitioners use gentle, specific adjustments to address the neurological interference. This isn’t an overnight process. Neuroplasticity, the brain’s ability to form new neural connections, drives the reorganization, and it takes time. But the trajectory is meaningful and measurable.
What Can Parents Do at Home for Tactile Defensiveness?
While working with professionals to address the underlying nervous system dysfunction, there are practical strategies that can help your child navigate daily life with tactile defensiveness:
- Use firm, predictable pressure. Light, unexpected touch is the most triggering for tactile-defensive children. When you touch your child, use steady, firm pressure rather than light ticklish contact. Warn them before you make physical contact.
- Respect their sensory boundaries. Believe your child when they say something hurts. Their nervous system is genuinely processing that input as painful or threatening. Forcing them to tolerate touch they find distressing doesn’t build resilience; it increases their nervous system’s threat response.
- Offer heavy work and deep pressure activities. Proprioceptive input—jumping, climbing, pushing, pulling, carrying heavy objects—provides calming input to the nervous system. Deep pressure activities like bear hugs (with permission), weighted blankets, and compression clothing can also help dampen tactile hypersensitivity.
- Modify clothing and grooming routines. Cut out all tags, choose soft fabrics, try socks without seams, and turn clothing inside out when seams cause distress. Break grooming tasks into smaller steps and give your child as much control over the process as possible.
- Reduce the overall sensory load. Tactile defensiveness worsens when the nervous system is already overwhelmed. Crowded, noisy, or visually stimulating environments compound the problem. Give your child regular access to quiet, low-stimulation spaces where their nervous system can recover.
- Don’t force exposure. Pushing a tactile-defensive child into contact with textures they find distressing doesn’t “toughen them up.” It activates their fight-or-flight response and can worsen their sensitivity over time. Let them explore textures at their own pace, with full control over when they stop.
Taking the Next Step for Your Child
Tactile defensiveness isn’t something your child chooses, and it’s not something you caused. It’s a signal from their nervous system that something deeper needs attention.
If your child’s touch sensitivity is affecting daily life—getting dressed, eating meals, tolerating grooming, accepting affection, or participating in activities with other children—their nervous system is asking for help.
The first step is getting a clear picture of what’s happening neurologically. PX Docs practitioners can run INSiGHT scans to identify the specific patterns of nervous system dysfunction driving your child’s sensory challenges, and build a customized care plan to address them at the root.
You don’t have to keep managing the symptoms while the underlying cause goes unaddressed. Your child’s nervous system has the capacity to change, and with the right support, it will.
Find a PX Docs practitioner near you by visiting the PX Docs Directory.
Frequently Asked Questions About Tactile Defensiveness
Can a Child Outgrow Tactile Defensiveness?
Some children’s nervous systems mature enough to partially compensate for tactile defensiveness over time, but many continue to experience touch sensitivity into adulthood. Rather than waiting to see if your child “grows out of it,” addressing the underlying nervous system dysfunction gives their brain the best opportunity to develop accurate sensory processing.
Is Tactile Defensiveness the Same as Sensory Processing Disorder?
Tactile defensiveness is one specific pattern within Sensory Processing Disorder, a broader condition that affects how the brain processes information from multiple senses. A child can have tactile defensiveness as their primary challenge, or it can appear alongside auditory sensitivity, vestibular issues, and other sensory processing differences.
How Is Tactile Defensiveness Diagnosed?
There’s no blood test or imaging study that diagnoses tactile defensiveness. Occupational therapists typically assess it through parent questionnaires, clinical observation, and standardized sensory profiles. INSiGHT scanning can also provide objective data on the patterns of nervous system dysfunction that underlie sensory processing challenges, giving families a clearer picture of what’s driving their child’s touch sensitivity.
Is Chiropractic Care Safe for Children with Tactile Defensiveness?
Neurologically-Focused Chiropractic Care for children uses gentle, precise adjustments—not the type of manual adjustments many adults associate with chiropractic. Pediatric adjustments are tailored to each child’s size, age, and neurological presentation, and PX Docs practitioners are specifically trained to work with children with sensory sensitivities.
What’s the Difference Between Tactile Defensiveness and Just Being “Picky”?
The key differences are the intensity and consistency of the reaction, and the degree to which it disrupts daily functioning. A child who prefers soft shirts but can wear others is expressing a preference. A child who has a full meltdown over a sock seam and can’t function until it’s removed is experiencing a neurological response; their brain is genuinely interpreting that input as threatening.
How Long Does It Take to See Improvement?
Every child’s nervous system responds on its own timeline. Some families notice changes in sleep, behavior, and sensory tolerance within weeks of beginning Neurologically-Focused Chiropractic Care. More complex cases—especially children with significant birth trauma history or multiple neurodevelopmental challenges—may need several months of consistent care before sensory processing improvements become apparent. INSiGHT scans often show neurological progress before outward symptoms visibly change.
At What Age Does Tactile Defensiveness Usually Appear?
Tactile defensiveness can appear as early as infancy, with signs like resisting being held, arching away from skin-to-skin contact, or becoming extremely distressed during bath time or diaper changes. It’s most commonly identified in toddlers and preschool-aged children when daily routines like dressing, grooming, and messy play become regular sources of conflict. Early identification matters because the nervous system is most adaptable during the first years of life.



