If your child has ADHD, there’s a good chance you’ve noticed something else: joints that bend a little too far, recurring ankle sprains, complaints of pain after activities other kids handle fine, or a body that seems both wired and exhausted at the same time. You may have brought it up with your pediatrician, only to hear that the two things aren’t related.
But they are. And the connection runs deeper than most parents and most doctors realize.
Research now shows that kids and adults with ADHD are significantly more likely to have joint hypermobility than the general population. The overlap isn’t a coincidence. It points to a shared root: a nervous system that’s been dysregulated from the start. At PX Docs, we see this pattern in practice constantly.
When we understand why ADHD and hypermobility so often travel together, we can stop chasing individual signs and start addressing what’s actually driving both.
What Is Joint Hypermobility?
Joint hypermobility refers to joints that move beyond their normal range of motion. Colloquially, these kids are called “double-jointed.” They can bend their thumbs to their wrists, hyperextend their knees and elbows, or fold themselves into positions that make other kids gasp. For some, this is just a benign trait. For many others, it comes with a real burden.
When hypermobility causes pain, fatigue, and other signs, doctors may diagnose Hypermobility Spectrum Disorder (HSD). A more severe form, Hypermobile Ehlers-Danlos Syndrome (hEDS), involves defects in collagen, the protein that gives connective tissues their structure and tensile strength. Because collagen is found in ligaments, tendons, skin, blood vessels, and gut tissue, hEDS and HSD can affect virtually every system in the body.
Common signs include:
- Joint pain and frequent sprains or subluxation
- Chronic fatigue
- Digestive issues like constipation and reflux
Dizziness upon standing (orthostatic intolerance) - Headaches
- Anxiety
- Difficulty with sleep
This wide sign range often leads to years of specialist appointments, each doctor looking at one piece without seeing the whole picture.
There are several connective tissue hypermobility conditions, each with distinct features. Clinicians assess hypermobility using the Beighton Scoring System, a 9-point scale measuring flexibility in specific joints. A score of 4 or higher typically indicates Generalized Joint Hypermobility (GJH).
What’s critical to understand is that hypermobility isn’t only a structural problem. The joints aren’t just loose; the nervous system’s ability to accurately sense where those joints are in space is impaired. That’s where the ADHD connection begins.
What the Research Says About ADHD and Hypermobility
The association between ADHD and joint hypermobility is no longer a clinical hunch. It’s well-supported by peer-reviewed research, and the numbers are striking.
A 2021 study of 431 adults with ADHD and 417 without ADHD found that those with ADHD were nearly five times more likely to have generalized joint hypermobility. When hypermobility came with additional musculoskeletal signs, what researchers call “symptomatic GJH”, the odds ratio climbed to nearly 7. The researchers concluded that GJH may represent a marker for an underlying systemic condition involving both connective tissue and the central nervous system.
A separate study found that 74% of children with ADHD showed generalized joint hypermobility, compared to just 13% of controls. Research from Brighton and Sussex Medical School found that over 50% of participants with a diagnosis of autism, ADHD, or a tic condition showed higher-than-average hypermobility levels. In a large Swedish population study, individuals with Ehlers-Danlos Syndrome were 5.6 times more likely to carry an ADHD diagnosis.
These aren’t minor correlations. They suggest that ADHD and hypermobility share foundational mechanisms, not just genetic coincidence.
There are proposed explanations for the overlap: shared genetic pathways affecting both collagen synthesis and dopaminergic neurotransmission, dysregulation of the Autonomic Nervous System affecting both attention and connective tissue inflammation, and proprioceptive deficits that impair both body awareness and brain regulation. Each of these threads ultimately leads back to the same place: the nervous system.
The Nervous System Is the Missing Link
Here’s what competitors discussing this topic consistently miss: the neurological bridge connecting ADHD and hypermobility isn’t abstract. It’s specific, measurable, and, critically, it can be addressed.
Proprioception
Proprioception is your body’s ability to sense where it is in space. It relies on sensory receptors in joints, muscles, and connective tissues that continuously send positional information to the brain. This input is foundational, not just for physical coordination; it’s a calming input that helps regulate the nervous system overall.
In children with joint hypermobility, loose ligaments and altered connective tissue mean the proprioceptive signal is noisy, unreliable, or outright impaired. The joints move too far, the receptors are stretched and strained, and the brain receives inconsistent information about the body’s position.
Children with ADHD independently show proprioceptive deficits too; their sense of body position is less accurate than that of neurotypical children. When you have both conditions, that proprioceptive disruption is compounded. The nervous system is running on a scrambled signal.
When proprioception goes down, something else goes up: nociception, the nervous system’s danger signaling. Less calming input means more alarm input. The brain stays activated, hypervigilant, and stuck in sympathetic overdrive. That’s the gas pedal pressed down, the brake pedal not working. That’s the dysregulated child who can’t sit still, can’t filter sensory input, can’t transition between activities, can’t settle down at night.
Dysautonomia
The Autonomic Nervous System controls the body’s involuntary functions, heart rate, blood pressure, digestion, temperature regulation, and immune response. When it’s working well, it shifts seamlessly between sympathetic (“gas pedal”) and parasympathetic (“brake pedal”) states based on what the situation demands.
Dysautonomia, dysfunction of the Autonomic Nervous System, is a recognized comorbidity of both ADHD and hypermobility. In hypermobile individuals, loose connective tissue can affect blood vessel walls, contributing to orthostatic intolerance and Postural Orthostatic Tachycardia Syndrome (POTS). POTS causes heart rate to spike and blood pressure to drop when moving from sitting to standing, resulting in dizziness, brain fog, and fatigue.
Research shows that roughly 20% of pediatric patients with POTS also have hypermobility conditions. POTS is increasingly recognized as a condition of autonomic dysregulation, and researchers have found that guanfacine, a medication used to treat ADHD, also helps manage POTS traits in many patients. The crossover in a care response tells us something important about shared neurological mechanisms.
When the Autonomic Nervous System is dysregulated, attention is fragmented, emotional regulation breaks down, sleep is disrupted, and the gut functions poorly. These aren’t separate signs; they’re expressions of a single system that’s lost its balance.
Why Do These Conditions Happen Together?
Conventional medicine looks at ADHD and hypermobility as separate diagnoses managed by different specialists. A psychiatrist handles the ADHD. A rheumatologist or geneticist handles the hypermobility. A gastroenterologist handles the digestive issues. A cardiologist evaluates the POTS. Each specialist sees their piece.
What none of them are asking is: why is this child’s nervous system in a state of chronic dysregulation across every system?
At PX Docs, we recognize that joint hypermobility conditions, including hEDS, are an explicit risk factor for subluxation. Subluxation isn’t a simple bone-out-of-place problem. It’s a neurological dysfunction characterized by three components:
- Misalignment in the neurospinal system
- Fixation and restricted motion in spinal segments
- Neurological interference that disrupts communication between the brain and body.
The key driver of neurological dysfunction in subluxation is impaired proprioception from the spinal joints themselves. When spinal joints don’t move normally, the brain receives distorted positional input from the spine, the most proprioceptively dense region of the body. That altered input disrupts sensory integration, autonomic regulation, and the brain’s ability to accurately process and respond to its environment.
Now consider what happens in a hypermobile child: loose ligaments allow spinal joints to shift out of their normal position and fail to stabilize properly. The very connective tissue laxity that makes joints hypermobile makes spinal subluxation more likely to develop and persist. And persistent subluxation creates ongoing neurological interference, a constant disruption in the brain-body communication circuit that the nervous system can’t compensate for indefinitely.
This is why hypermobile children so frequently develop ADHD-like signs: inattention, hyperactivity, sensory dysregulation, emotional dysregulation, poor sleep, and digestive dysfunction.
The “Perfect Storm” of How This Starts Before the Diagnosis
Understanding why a specific child develops both hypermobility and ADHD requires stepping back even further, before the school-age years, before the toddler tantrums, often before birth itself.
At PX Docs, we describe this through the “Perfect Storm” framework. This concept explains how a series of early life stressors accumulate during the most neurologically sensitive windows of development, creating conditions for chronic nervous system dysfunction.
Stage 1: Prenatal and Fertility Stress
Modern pregnancies often involve fertility interventions, significant maternal stress, and elevated cortisol levels throughout gestation. That stress doesn’t stay with the mother; it crosses the placenta. The developing nervous system is bathed in stress hormones during the most impressionable period of its formation. The baby’s nervous system doesn’t learn balance; it learns survival mode.
For children with a genetic predisposition to connective tissue differences, which hypermobility syndromes have a hereditary component, prenatal stress during this window may amplify the developmental impact of that predisposition.
Stage 2: Birth Trauma and Interventions
The upper cervical spine and brainstem region are the most neurologically vulnerable areas of the body. During labor and delivery, interventions like forceps, vacuum extraction, prolonged pushing, or C-section delivery can apply significant force to this region. Even uncomplicated deliveries involve forces on the infant’s neck that, in a child with connective tissue laxity, are more likely to result in spinal subluxation.
Birth trauma to the upper cervical spine directly affects the brainstem, the master regulator of the Autonomic Nervous System, and the gateway for the vagus nerve. Vagus nerve dysfunction from birth trauma impairs the parasympathetic brake. The infant enters the world with the gas pedal already partially stuck down.
In hypermobile infants, the loose ligament laxity that characterizes their connective tissue means the upper cervical subluxation from birth is both more likely to occur and harder for the body to stabilize on its own. This creates a neurological foundation for the dysregulation that will manifest as ADHD, sensory processing challenges, anxiety, and the full spectrum of traits we see in these children.
Stage 3: Early Childhood Stressors
Colic, chronic ear infections, antibiotic use, poor sleep, and feeding difficulties are the early warning signs that a child’s nervous system is already struggling. Conventional medicine cares for each trait in isolation. What we recognize is that these are the early expressions of subluxation-driven nervous system dysregulation. The neurology doesn’t change; medicine just gives it a different diagnosis at each developmental stage.
The proprioceptive disruption from subluxation, compounded by the inherent proprioceptive impairment of connective tissue hypermobility, creates a nervous system that can never fully regulate. By the time these children reach school age, the ADHD diagnosis is almost inevitable.
Signs That Your Child’s ADHD and Hypermobility Share a Neurological Root
Not every child with ADHD and hypermobility has this pattern, but there are specific signs that suggest a shared neurological root rather than two separate conditions happening to coincide:
- Sensory processing difficulties alongside joint signs. Children who are both hypermobile and have sensory processing difficulties, avoiding certain textures, sounds, or lights, or craving deep pressure and heavy input, are showing proprioceptive dysregulation at a nervous system level, not just in the joints.
- Fatigue that doesn’t match activity level. Hypermobile children with ADHD often crash hard. The body and nervous system are working overtime to maintain joint stability and regulate attention simultaneously. Unexplained fatigue after normal activity is a signal that the Autonomic Nervous System is overloaded.
- Digestive issues alongside behavioral signs. Constipation, bloating, reflux, or irritable bowel signs in an ADHD and hypermobile child point to vagus nerve dysfunction. The vagus nerve controls both gut motility and emotional regulation through its parasympathetic pathways.
- Poor response to standard ADHD interventions alone. If behavioral strategies, medication, and therapy have only partially helped, and the child still struggles with emotional dysregulation, sleep, and physical traits, the neurological root hasn’t been addressed.
- A history that includes difficult birth, early colic, or frequent infections. This is the “Perfect Storm” history. These aren’t unrelated early events; they’re the sequence that sets the neurological stage for everything that follows.
How Neurologically-Focused Chiropractic Care Addresses the Root
Neurologically-Focused Chiropractic Care isn’t about cracking backs or caring for joint pain. It’s specifically directed at the subluxation-driven neurological interference that underlies the conditions described in this article.
The first step is objective assessment. PX Docs practitioners use INSiGHT scans, a technology that measures nervous system function through:
- NeuroThermal scans
- Surface electromyography (sEMG)
- Heart Rate Variability (HRV) analysis.
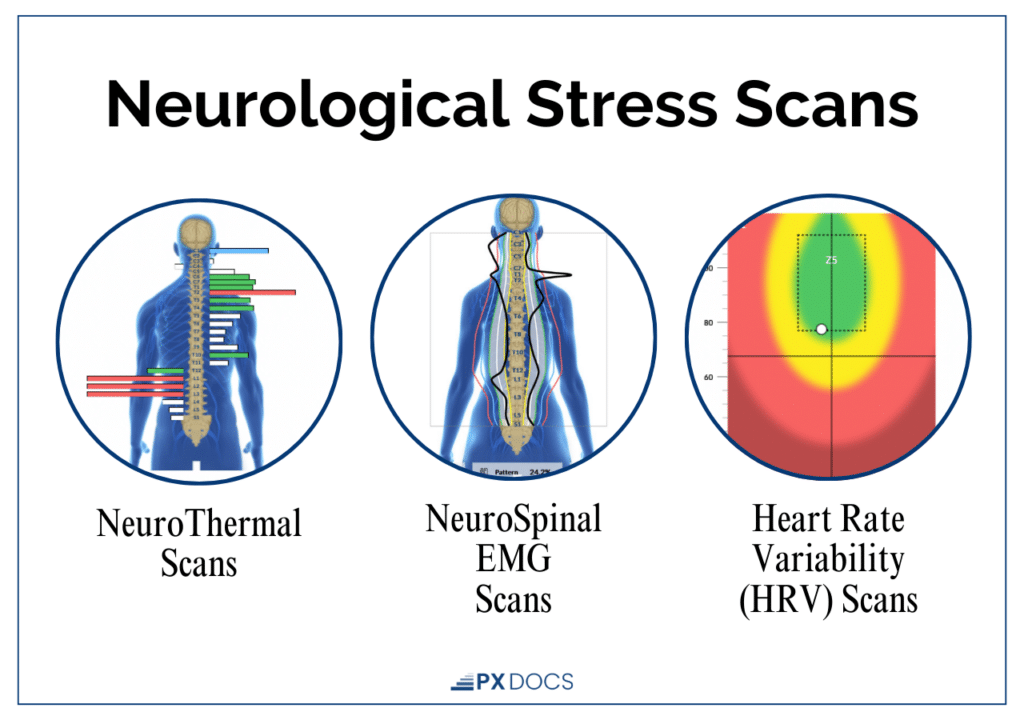
These scans don’t diagnose conditions; they objectively reveal where and to what extent the nervous system is dysregulated, showing the patterns of autonomic imbalance and neurological interference that can’t be seen on standard imaging or detected through routine medical exams.
For a child with both ADHD and hypermobility, INSiGHT scans often reveal significant dysautonomia patterns, chronic sympathetic dominance, suppressed parasympathetic tone, and altered sensorimotor function concentrated in the upper cervical spine and brainstem region. This is the objective neurological picture of what the child and family have been experiencing subjectively for years.
From there, gentle and specific Neuro-Tonal adjustments are directed at the subluxated segments, restoring proper movement, improving proprioceptive input from the spine, and allowing the Autonomic Nervous System to shift back toward balance. In a hypermobile child, this requires particular care and precision, since the goal isn’t simply mobilizing joints (which are already mobile) but restoring neurological function in segments that are fixated and neurologically disrupted.
What to Expect: The Healing Timeline
Parents should understand that addressing a nervous system that’s been dysregulated since birth takes time. There’s no quick fix. Healing follows a sequence: the Autonomic Nervous System begins to regulate before behavioral and cognitive changes become obvious. Sleep often improves first. Digestive function normalizes. Emotional dysregulation decreases. Attention and sensory processing improve as the neurological foundation becomes more stable.
For children with hypermobility and ADHD, the timeline is typically 3–12 months of consistent neurologically-focused care to see substantial improvement in the full trait picture. This is real, lasting change at the level of the nervous system, not trait management, but actual neurological restoration.
You Don’t Have to Manage Two Separate Conditions
If your child has both ADHD and joint hypermobility, you’ve probably been told to manage each one separately. Different appointments, different specialists, different interventions, none of them talking to each other.
But these conditions aren’t separate. They share a common neurological root: a nervous system that learned dysregulation early, driven by the accumulation of stressors through the “Perfect Storm,” and sustained by ongoing neurological interference from subluxation.
When you address the root, both conditions respond.
Neurologically-Focused Chiropractic Care isn’t a replacement for the pediatrician, the occupational therapist, or the mental health support your child may already be receiving. It’s the missing foundation, the piece that restores the nervous system’s capacity to regulate, so every other intervention works better. If your child fits this picture, we encourage you to find a PX Docs provider near you. A thorough neurological assessment, starting with INSiGHT scanning, can show you exactly what’s happening in your child’s nervous system and what’s possible when it’s addressed at its root.