

Approximately 470,000 children in the United States live with epilepsy, with Juvenile Myoclonic Epilepsy (JME) accounting for up to 10% of all cases. Numbers alone, though, can’t capture what it’s like to watch your teenager experience a seizure for the first time.
When seizures suddenly enter your child’s life, everything changes in an instant. One morning, you’re waking up your teenager for school, the next, you’re rushing to the ER after a seizure you never saw coming. The fear, the endless “what ifs,” and the weight of hearing words like ‘genetic’ and ‘lifelong condition’ can leave any parent and child feeling powerless.
But here’s what often gets left unsaid: seizures don’t just appear out of nowhere. For many kids, especially those diagnosed with Juvenile Myoclonic Epilepsy, these episodes are the result of a long build-up of stress on the nervous system. What seems sudden is often the final straw of what we call The Perfect Storm.
This article isn’t another list of seizure types or medications. Instead, it’s about understanding what’s really happening in your child’s brain and body—and exploring a path that goes deeper than just managing symptoms, toward actually addressing the root causes contributing to Juvenile Myoclonic Epilepsy.
What Is Juvenile Epilepsy?
Juvenile epilepsy includes several seizure conditions that typically begin between the ages of 12 and 18. The most common type, juvenile myoclonic epilepsy (JME), affects 5-10% of all epilepsy cases. Unlike childhood epilepsy, these seizures often appear suddenly in healthy teenagers, leaving families desperate for answers.
Think of epilepsy as an electrical storm in the brain. When your nervous system can’t maintain proper balance, groups of nerve cells fire abnormally, causing seizures. What makes juvenile epilepsy unique is its timing, appearing during adolescence when the brain undergoes massive rewiring and development.
JME specifically involves three seizure types: myoclonic seizures (quick muscle jerks), absence seizures (brief staring spells), and generalized tonic-clonic seizures (full-body convulsions). While JME is most common, other forms include juvenile absence epilepsy and epilepsy with generalized tonic-clonic seizures on awakening.
What conventional medicine tends to overlook is that the teenage brain’s vulnerability isn’t just genetic. It’s about accumulated stress reaching a tipping point. The hormonal changes, sleep deprivation, overuse of technology, academic pressure of adolescence, and more can unmask nervous system dysregulation that’s been building since birth.
Recognizing the Signs
Understanding different seizure types helps you recognize what’s happening and communicate effectively with doctors. Each type has distinct characteristics, though many teenagers with JME experience all three.
Myoclonic Seizures: The Morning Jerks
These brief, shock-like muscle jerks are JME’s hallmark, affecting both arms simultaneously. Parents often first notice their teen dropping breakfast items, spilling drinks, or seeming unusually clumsy. These jerks happen within 1 to 2 hours of waking and last just a fraction of a second.
The morning timing makes sense neurologically. Upon waking, your nervous system shifts from parasympathetic dominance (rest, regulate, and digest mode) to sympathetic activation (alert mode). In teens with nervous system dysfunction, this transition can trigger abnormal electrical activity.
Absence Seizures: Beyond Daydreaming
During these 10-second episodes, your teenager stares blankly, doesn’t respond to their name, and has no memory of it afterward. Teachers often mistake these for daydreaming, delaying diagnosis. Unlike childhood absence epilepsy, JME absence seizures may include subtle eyelid fluttering or head nodding.
Generalized Tonic-Clonic Seizures
Affecting 80% of teens with JME, these seizures involve sudden unconsciousness, body stiffening, and then rhythmic jerking. They typically last 1-3 minutes and commonly occur upon waking or when sleep-deprived. Many are preceded by clusters of myoclonic jerks—a warning sign families learn to recognize.
Beyond these primary types, watch for increased anxiety, mood changes, morning difficulties, light sensitivity (affecting 30% with JME), and coordination problems that worsen with stress.
What Really Causes Juvenile Epilepsy?
Medical textbooks cite genetics, noting 50% of cases show family history. But genetics load the gun—the environment pulls the trigger. Understanding true root causes requires examining the complex interplay between genetic susceptibility and accumulated neurological stressors.
Beyond Genetics: Why Environment Matters More
Yes, genes like GABRA1, CACNB4, and EFHC1 are associated with JME. But having these variations doesn’t guarantee epilepsy. Epigenetics shows that environmental factors determine whether these genes express themselves. Identical twins sharing 100% DNA don’t always both develop epilepsy—clear proof genetics isn’t destiny.
Why does epilepsy suddenly appear in teenage years if it’s purely genetic? The answer: neurological stress accumulates over time, eventually overwhelming your nervous system’s balance.
The “Perfect Storm” of Multiple Factors Creating Vulnerability
We’ve observed consistent patterns in thousands of children who develop juvenile epilepsy, a “Perfect Storm” beginning much earlier than the first seizure:
- Prenatal Stress and Birth Trauma: Pregnancy complications and prenatal maternal psychological distress impact early brain development. Prolonged labor, C-sections, forceps, vacuum extraction, or oxygen deprivation stress the infant’s brainstem and upper cervical spine—areas crucial for nervous system regulation. This early birth trauma can create subtle dysfunction that doesn’t fully manifest until adolescence.
- Early Childhood Stressors: Following birth trauma, many children experience cascading challenges: colic, chronic ear infections, digestive issues, and delayed milestones. Multiple antibiotics disrupt the gut-brain connection, while chronic illness keeps the nervous system stressed. These kids often struggle with sensory processing or attention—signs of underlying nervous system dysfunction.
- The Adolescent Tipping Point: During puberty, massive brain reorganization occurs. Hormonal surges, academic pressure, social stress, technology overuse, anxiety, and chronic sleep deprivation push an already vulnerable nervous system past its threshold. Teenagers need 8-10 hours of sleep, yet most get far less, exhausting a struggling nervous system.
This “Perfect Storm” explains why some genetically predisposed children never develop epilepsy, while others without genetic markers do. More importantly, it reveals intervention opportunities beyond medication.
The Hidden Neurological Connection: Dysautonomia and Vagus Nerve Dysfunction
While conventional neurology focuses on brain waves, the real story involves your Autonomic Nervous System—specifically, the balance between sympathetic (fight-or-flight) and parasympathetic (rest, regulate, and digest) function. This imbalance, called dysautonomia, creates conditions that make seizures more likely.
Think of your Autonomic Nervous System as your body’s autopilot. In teens with epilepsy, we consistently see the sympathetic system stuck in overdrive (gas pedal floored) while the parasympathetic system, controlled by the vagus nerve, is underactive (faulty brakes).
Parents often notice related signs they don’t connect to epilepsy: chronic constipation, temperature regulation problems, excessive anxiety, poor sleep quality, and extreme stress reactions. These aren’t separate issues—they’re all dysautonomia signs contributing to seizure activity.
The Vagus Nerve
The vagus nerve, your longest cranial nerve, skillfully regulates the parasympathetic system. Running from the brainstem, through the neck, into the chest and abdomen, it influences everything from heart rate to inflammation. When functioning properly, it maintains electrical stability that prevents seizures.
However, when compromised, often from birth trauma affecting the upper cervical spine, the vagus nerve can’t counterbalance sympathetic overdrive. This explains why many teens with JME also have inflammation, gut issues, and stress recovery problems.
The medical community recognizes this connection, using Vagus Nerve Stimulation (VNS) for medication-resistant epilepsy, but many parents come to us feeling that it is invasive, unreliable, or ineffective over time.
What makes our approach unique is identifying and addressing vagus nerve dysfunction before surgical intervention becomes necessary. We can measure function and pinpoint where the nervous system becomes dysregulated, which, when addressed, significantly impacts seizure threshold.
Understanding and Managing Triggers
While most resources list triggers superficially, understanding the mechanisms empowers strategic prevention.
Sleep Deprivation
Sleep deprivation is JME’s most powerful trigger, but it’s not just being tired. During sleep, your brain clears metabolic waste, consolidates pathways, and resets neurotransmitters. Without adequate sleep (8-10 hours for teens), these processes remain incomplete. The sleep-deprived brain operates with accumulated waste, imbalanced neurotransmitters, and compromised inhibitory mechanisms—essentially, the neurological brakes preventing excessive electrical activity go offline.
Creating a sleep sanctuary involves more than earlier bedtimes. Blue light suppresses melatonin, which means that evening screens have a direct impact on sleep quality. Room temperature matters too—60-67°F optimizes sleep. Most importantly, consistent sleep-wake times, even on weekends, regulate circadian rhythm.
Stress and Hormones
Stress floods your body with cortisol and adrenaline, increasing neuronal excitability and lowering seizure threshold. For teenage girls, menstrual cycles create vulnerability windows—estrogen increases excitability while progesterone has anticonvulsant properties. Even electromagnetic fields from devices can influence neuronal firing in sensitized nervous systems.
Diagnosis and Assessment: Beyond the EEG
While EEG remains the standard medical test for epilepsy, showing characteristic 3-6 Hz polyspike patterns in JME, it’s common for people with epilepsy to have normal EEGs between seizures. It only captures a brief snapshot—like photographing the ocean to understand all its currents.
What’s also important to note is that EEGs don’t measure autonomic function, vagus nerve tone, or accumulating neurological tension preceding seizures. They don’t explain why that irregular electrical activity is happening in the first place.
Unfortunately, many families walk away from an EEG with a diagnosis and are handed medications with potentially significant side effects, often without anyone looking deeper at what’s foundationally causing the seizures. While these medications can help manage symptoms, they don’t address the underlying nervous system stressors that contributed to the problem in the first place.
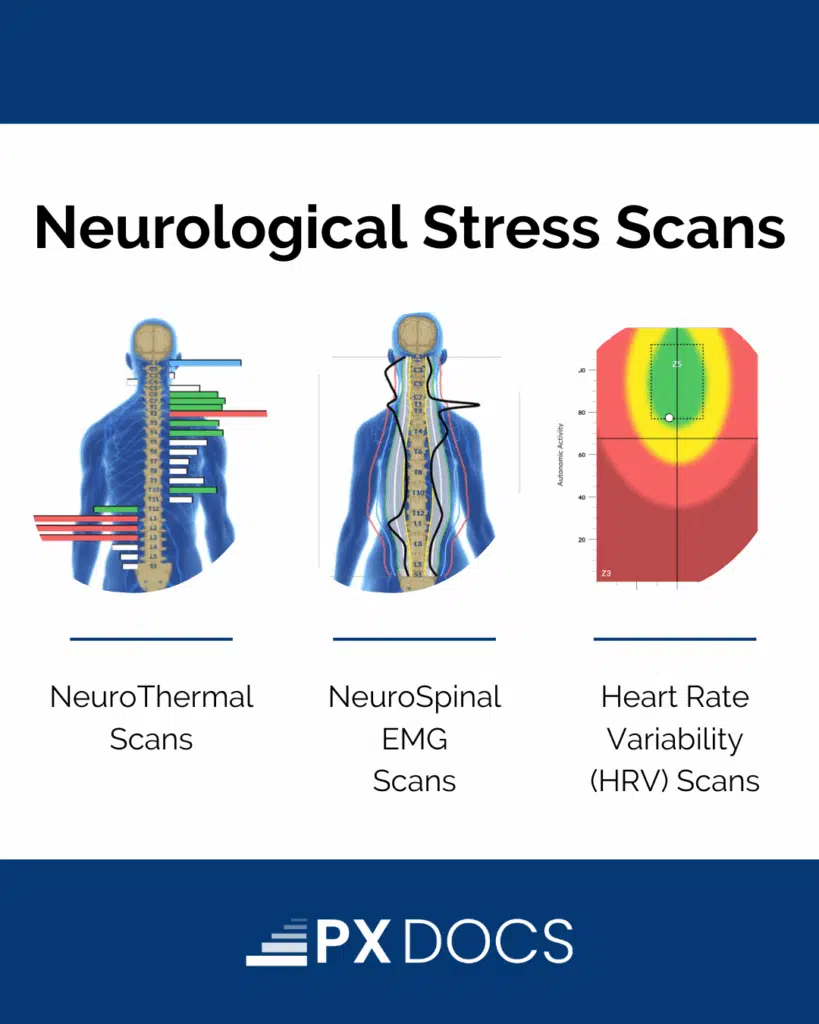
INSiGHT Scanning: Measuring Nervous System Function
At PX Docs, we utilize INSiGHT scanning technology to measure aspects of nervous system function directly relating to seizure susceptibility. Unlike standard tests, it helps identify the underlying dysfunction driving the seizures, giving parents real answers and a roadmap for addressing the root causes—not just managing symptoms
Thermal scans reveal where the nervous system is stuck in sympathetic overdrive. Heart rate variability assessments evaluate vagus nerve function and stress adaptation—low HRV indicates reduced resilience and increased vulnerability. EMG scans identify chronic neuromuscular tension patterns indicating sustained stress.
These scans often reveal dysfunction years before seizures begin and show measurable improvement as balance is restored.
During care, these scans serve as an essential clinical guide for PX doctors, enabling them to tailor the care plan and adjust techniques to the individual child. Families love being able to see the nervous system changing over time and notice how these objective improvements often align with reductions in seizure activity and positive shifts at home.
Parents frequently report early changes in everyday life—better sleep, calmer moods, and smoother digestion—while, over time, thousands of children have experienced significant reductions in seizures, with many achieving complete resolution, all while working closely with their PX doctors to address the root neurological dysfunction.
Care Approaches Beyond Medication
While medications (valproate, lamotrigine, levetiracetam) can be important, they try to suppress the seizures without addressing why the nervous system destabilized in the first place. Many teens require increasing doses or multiple medications over time.
Natural Support to Enhance Nervous System Function
What if we could improve your child’s nervous system’s self-regulation ability?
Neurologically-Focused Chiropractic Care addresses root neurological dysfunction through specific adjustments targeting subluxation that keeps the nervous system stuck in sympathetic overdrive. These precise, gentle neurotonal adjustments remove nervous system interference, allowing the nervous system to regulate more effectively and efficiently on its own.
Natural vagus nerve stimulation includes specific breathing exercises, cold exposure, humming, and gentle neck stretches. Nutritional support with omega-3s, magnesium, and B-vitamins while avoiding inflammatory foods can also help reduce seizure frequency.
Your Next Steps Forward
While seizures manifest in the brain, they often begin in a nervous system overwhelmed by accumulated stress. The “Perfect Storm” creating vulnerability can be addressed. Nervous system function can be restored. Your child’s seizure threshold can improve.
Understanding juvenile epilepsy stems from neurological dysfunction rather than genetic inevitability changes everything. Yes, work closely with a trusted neurologist. But addressing root causes through nervous system regulation offers hope beyond seizure suppression.
If you’re ready to explore how Neurologically-Focused Chiropractic Care can complement your child’s epilepsy management, visit the PX Docs Directory to find a qualified practitioner who understands the nervous system-seizure connection.
Your teenager’s diagnosis doesn’t have to be their destiny.



