

Your child wakes up again, clutching their head. The light hurts, and they feel sick to their stomach. You’ve already cut out chocolate, kept their bedtimes consistent, and ensured they’re drinking enough water, but the migraines keep coming. You’re doing everything the pediatrician told you to do. So why isn’t it working?
Triggers don’t cause migraines. They set them off in a nervous system that was already vulnerable. And if you want to understand what causes migraines in children at the root level, not just which foods or sleep patterns make them worse, you need to look deeper. You need to look at the neurological foundation underneath.
This article covers the standard triggers, the actual brain mechanisms behind pediatric migraines, and why some children are far more susceptible than others, including what the research says about the Autonomic Nervous System’s role. By the end, you’ll have a much clearer picture of what’s really driving your child’s migraines, and what you can actually do about it.
What Is a Migraine in Children?
Migraine is not a bad headache. It’s a neurological condition, one that affects roughly 10% of school-age children and accounts for up to 18% of pediatric emergency room visits.
Migraines in children look different from those in adults. Adults often describe a unilateral, throbbing pain lasting 4–72 hours. Kids can have attacks that are bilateral, shorter in duration (sometimes as little as one hour), and more closely tied to nausea, vomiting, and stomach pain. Some younger children experience what’s called an abdominal migraine, stomach pain without any headache at all.
A typical migraine moves through up to four stages.
- In the prodrome phase, occurring 24 hours before an attack, some children become irritable or fatigued, develop a stiff neck, or have food cravings; this is estimated to affect over two-thirds of children.
- The aura phase, experienced by about one-third of migraine patients, brings visual, sensory, or motor disturbances before the headache starts, flashing lights, numbness, or trouble with speech. This affects roughly 5% of adolescents.
- Then comes the headache phase itself: the full attack with nausea, vomiting, and light and sound sensitivity lasting anywhere from one to 72 hours without care.
- After the pain clears, the postdrome phase can leave a child exhausted, moody, or mentally foggy for hours or even days.
Migraine is also significantly associated with conditions like ADHD, anxiety, and allergic rhinitis, a connection that points to something deeper than just head pain.
Common Migraine Triggers in Children
Every list of what causes migraines in children starts here, and for good reason. Identifying and managing triggers is a legitimate strategy for reducing attack frequency. The most common triggers include:
- Sleep disruption. Too little sleep, too much sleep, or an inconsistent schedule can all set off an attack. Lack of sleep and poor sleep quality are among the most consistently cited triggers across all age groups.
- Stress. Emotional stress is a major driver, including schoolwork, social conflict, over-scheduling, and major life changes. And this is often overlooked: it doesn’t have to be negative stress. Even exciting events can trigger a migraine in a susceptible child.
- Dehydration. Children who don’t drink enough water throughout the day significantly raise their risk of attack. By the time a child feels thirsty, they’re already mildly dehydrated.
- Skipping meals or low blood sugar. Missing meals or going too long between eating disrupts blood sugar regulation and is a well-documented trigger. Consistent, whole-food meals matter.
- Food and food additives. Specific foods commonly linked to migraines include caffeine, chocolate, aged cheeses, processed meats, MSG, artificial sweeteners, and foods high in histamines, such as fermented foods and dried fruits. Every child’s sensitivities differ.
- Screen time and sensory overload. Extended screen use contributes to eye strain, overstimulation, and disrupted sleep, all of which increase the risk of attacks. This is especially relevant for children already dealing with sensory sensitivities.
- Weather and barometric pressure changes. Shifts in atmospheric pressure, temperature, and humidity are consistently reported triggers, particularly in children who seem to get migraines around weather changes.
- Hormonal changes. For adolescent girls, migraine frequency often increases around the onset of menstruation. Females are three times more likely than males to experience migraines once puberty begins.
Tracking these triggers through a headache diary is genuinely useful; logging when attacks happen, what preceded them, and how long they last can reveal patterns that make avoidance practical. But avoiding triggers is reactive management, not resolution.
What Actually Causes Migraines?
The honest answer from neuroscience is that the exact cause of migraines is still being worked out. What researchers do know is that migraines are not simply vascular events. The older model, that migraines are caused by dilated blood vessels, has largely been replaced.
The current understanding centers on Cortical Spreading Depression (CSD): a wave of electrical activity that moves across the cortex and temporarily disrupts normal brain function. This is what produces the aura in many patients. Following this wave, the trigeminal nerve system becomes activated, releasing inflammatory peptides that cause the characteristic throbbing pain.
Changes in neurotransmitters, particularly serotonin, dopamine, and glutamate, are heavily involved in this process. Research indicates that fluctuations in serotonin levels appear to help drive the neurochemical changes that trigger attacks.
Critically, migraine is now understood as a condition of neurological sensitivity, a brain that is hyperreactive to stimuli that a non-migraine brain processes without incident. This is why the same stressor that gives your child a migraine might not affect another child at all. The difference isn’t the trigger. It’s the underlying neurological state.
And this is where conventional medicine’s trigger-focused approach runs into its ceiling.
Why Some Children Get Migraines and Others Don’t
This is the question that most migraine articles never answer: why is one child’s nervous system so reactive to triggers that another child handles without any problem?
The answer lies in the Autonomic Nervous System, specifically, the balance between its two branches.
Think of it this way: your child’s Autonomic Nervous System has two primary modes:
- The Sympathetic Nervous System branch is the “gas pedal”; it drives the fight-or-flight response.
- The Parasympathetic Nervous System branch is the “brake pedal”; it handles rest, recovery, and regulation.
In a healthy nervous system, these two systems balance each other dynamically, responding to demands and returning to a state of calm.
In children with chronic migraines, research demonstrates Autonomic Nervous System dysfunction. A separate study of pediatric headache patients found significantly higher frequencies of autonomic signs, insomnia, dizziness, and cold extremities in children with migraine compared to controls. When the nervous system is stuck too close to the gas pedal, with chronically elevated cortisol and a system perpetually on alert, the threshold for an attack drops.
When a trigger arrives, it lands on a nervous system with almost no reserve capacity left. The migraine isn’t caused by the missed meal or the stressful test day. Those are the last straws on a system already operating at its limit.
This autonomic imbalance, also called dysautonomia, doesn’t just affect migraine susceptibility. It connects to the other signs many migraine kids carry: disrupted sleep, digestive issues, anxiety, and mood instability. These are all downstream effects of a nervous system that can’t properly regulate itself.
The Vagus Nerve’s Role in Pediatric Migraines
One of the most important, and most underexplained, pieces of the pediatric migraine puzzle is the vagus nerve.
The vagus nerve is the primary nerve of the parasympathetic system. It runs from the brainstem all the way through the heart, lungs, and digestive tract, coordinating a massive range of regulatory functions. When the vagus nerve is functioning well, it acts as the body’s primary brake, calming the stress response, regulating heart rate, reducing inflammation, and keeping the system balanced.
The vagus nerve’s connection to migraines is well established in the research. The autonomic nerve and its direct connections with the vagus nerve in the brainstem form the basis of the head’s pain pathways, and these pathways can be modulated through vagal stimulation, inhibiting the trigeminocervical neuron firing that drives migraine pain.
This mechanism is exactly why the FDA cleared a noninvasive vagus nerve stimulation device for acute migraine care in 2018. A 2025 case report in Frontiers in Pain Research documented significant reductions in attack frequency and complete aura resolution in an 8-year-old with chronic migraine after vagal stimulation, early evidence that improving vagal function directly impacts migraine outcomes in children.
In children with low vagal tone, the parasympathetic brake doesn’t engage strongly enough to counteract sympathetic activation. The nervous system can’t “come back down” between stressors. The threshold for triggering a migraine drops, and recovery time after each attack gets longer.
What damages vagal tone in children? This is where the story goes back further than most people expect.
The “Perfect Storm”: Why Your Child’s Nervous System Was Already Vulnerable
Most articles on what causes migraines in children start the story at the migraine itself, the triggers, the signs, and the attack. But the neurological vulnerability that makes a child susceptible to chronic migraines often begins much earlier. We call this the “Perfect Storm.”
The “Perfect Storm” is a sequence of early life stressors that accumulate and interact, creating neurological dysfunction that shows up years later as chronic health challenges, including migraines.
- It starts before birth. When a mother experiences significant prenatal stress, anxiety, or health challenges during pregnancy, stress hormones like cortisol cross the placenta and directly affect the developing nervous system. A baby exposed to chronic cortisol begins developing with a bias toward sympathetic dominance, a nervous system already tilted toward fight-or-flight before the child takes a single breath.
- Then comes birth. Birth interventions, C-sections, forceps, vacuum extraction, prolonged labor, induction, and applying significant mechanical force to the infant’s upper neck and brainstem region. This is where the vagus nerve exits the skull. Physical stress to this region can cause subluxation, neurological interference, and dysfunction in the upper cervical spine, disrupting normal brainstem and autonomic function. Even a “normal” delivery involves intense compressive forces on a newborn’s delicate neurospinal system.
- Early childhood adds more load. Frequent ear infections, rounds of antibiotics, food sensitivities, chronic illness, excessive screen time, falls, and sports injuries are all neurological stressors that pile onto a system already operating with reduced capacity. Each one chips away at the reserve.
The result, years later, is a child whose nervous system is chronically dysregulated, stuck in sympathetic dominance, with impaired vagal tone and a low threshold for neurological reactivity. When migraine triggers arrive, the system has nowhere left to go.
An attack is the output of a nervous system that has exhausted its adaptive capacity.
What Conventional Medicine Gets Right
Conventional pediatric neurology does important work. Proper diagnosis matters. Ruling out secondary causes, such as brain tumors, structural abnormalities, and inflammatory conditions, is critical and should always happen when a child presents with new or changing headache patterns. Preventive medications and acute care options are real tools that can reduce suffering for many children.
The trigger management approach works, partially. It reduces attack frequency by lowering the load on an already-vulnerable nervous system. Consistent sleep, hydration, regular meals, and stress management all support neurological function regardless of the underlying cause.
Where conventional medicine falls short is in asking why this child’s nervous system is so sensitive to begin with. The standard evaluation doesn’t examine autonomic balance, vagal function, or neurospinal integrity.
There’s no blood test that reveals sympathetic dominance, and no standard scan that identifies subluxation-related neurological dysfunction. So the underlying pattern goes unchecked, and families find themselves managing triggers indefinitely rather than addressing the root cause.
How Neurologically-Focused Chiropractic Care Approaches Pediatric Migraines
This is where Neurologically-Focused Chiropractic Care comes in, not as an alternative to proper medical care, but as a root-cause approach that works on the neurological foundation conventional medicine doesn’t address.
It’s important to be clear: this technology does not diagnose medical conditions, and Neurologically-Focused Chiropractic Care is certainly not a treatment or cure for migraines in children or any other condition, not even back pain. Instead, INSiGHT Scans help track down the root cause of nervous system dysfunction and dysregulation, and build customized care plans and adjust protocols to help shift the nervous system back into a state of balance, regulation, and resilience.
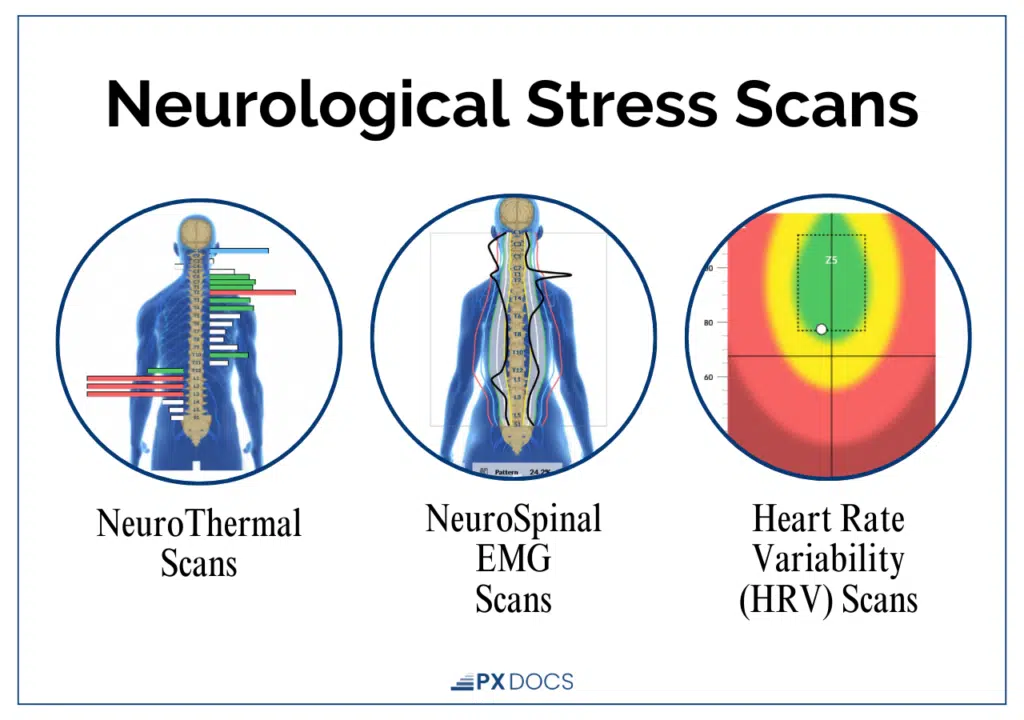
The INSiGHT scanning system measures three aspects of neurological function.
- Thermal scanning uses infrared sensors to detect temperature asymmetries along the spine, a marker of Autonomic Nervous System dysregulation and inflammation associated with subluxation.
- Surface electromyography (sEMG) assesses the electrical activity in the neurospinal muscles, revealing areas of chronic neuromotor tension and dysfunction.
- Heart Rate Variability (HRV) analysis measures the balance between the sympathetic and parasympathetic branches of the Autonomic Nervous System, providing an objective picture of where a child sits on the gas-to-brake spectrum.
For many parents of children with chronic migraines, these scans are the first time they’ve seen an objective picture of their child’s nervous system function. They often show a system running hot, elevated sympathetic activity, reduced parasympathetic capacity, and neurological tension patterns that align with what the research shows about migraine susceptibility.
Neurologically-Focused Chiropractic Care then works to reduce subluxation, the neurological interference, restoring more balanced communication between the brain, brainstem, and body. As the nervous system shifts toward better regulation, the parasympathetic brake engages more effectively, vagal tone improves, and the neurological threshold for migraine becomes harder to reach.
It’s important to note that Neurologically-Focused Chiropractic Care takes a fundamentally different approach to external vagal nerve stimulation, focusing on restoring function rather than just activating it. While external stimulation may temporarily “turn on” the vagus nerve, it doesn’t address why that nerve isn’t working properly in the first place.
Neurologically-focused care works to identify and gently remove that interference, allowing the vagus nerve to regulate, adapt, and respond as it was designed to. Instead of relying on ongoing external input, the goal is to help the body regain its own internal balance—so healing, regulation, and resilience can happen from within.
What Parents Can Do Right Now
While you’re exploring root-cause approaches, these strategies reduce attack frequency by supporting nervous system regulation.
Protect sleep ruthlessly: consistent bedtime, consistent wake time, and a dark, quiet environment. Sleep is when the parasympathetic system does its deepest repair work. Keep blood sugar stable with regular meals containing protein, fat, and fiber, and don’t let kids skip breakfast. Prioritize hydration throughout the day, not just when they complain of thirst. Reduce nervous system load by addressing the biggest stressors: screen time, over-scheduling, sensory overload, and chronic unmanaged stress. Keep a headache diary, logging when attacks happen, what preceded them, sleep quality, food, stress events, and weather. Patterns emerge over weeks that aren’t obvious day-to-day.
And have a proper neurological evaluation. Any new headache pattern in a child, or one that is increasing in frequency or severity, warrants evaluation by a healthcare provider to rule out secondary causes.
Next Steps
What causes migraines in children is a more complex question than the standard trigger lists suggest. Yes, sleep disruption, stress, dehydration, and food sensitivities trigger attacks. But they set attacks off in a nervous system that’s already running on the edge, one where sympathetic dominance has reduced the threshold for neurological reactivity, where vagal tone is low, and where the brain can’t adapt to normal stressors the way it should.
Understanding the “Perfect Storm,” how prenatal stress, birth trauma, and early childhood stressors compound over time to create chronic nervous system dysregulation, changes the entire conversation. It shifts the focus from “what triggered this attack” to “why is my child’s nervous system so vulnerable to begin with?”
That’s the question worth asking. And that’s the question Neurologically-Focused Chiropractic Care is built to answer. If your child struggles with chronic or recurrent migraines, consider connecting with a PX Docs practitioner who can perform a full neurological assessment and help you understand the root cause pattern driving the problem. Find a provider near you in the PX Docs provider directory.



