

Neurostorming is a state of extreme Autonomic Nervous System dysregulation in which the sympathetic “fight or flight” response surges out of control, most often after a traumatic brain injury. In the medical literature, neurostorming is also called Paroxysmal Sympathetic Hyperactivity (PSH), and it produces episodes of racing heart rate, fever, soaring blood pressure, sweating, and rigid muscle posturing. It’s most common in children with severe brain injuries, hypoxic-ischemic encephalopathy, or significant birth trauma, and it’s deeply distressing for the families living through it.
When I first met little Scarlett, a newly turned one-year-old girl struggling with seizures, neurostorming, and significant developmental delays triggered by a stressful pregnancy and rough labor and delivery, the number one thing impacting her sleep and daily quality of life was her neurostorming. Then, compounding the issue, her medical team had her loaded up on multiple heavy-hitting medications from Vigabatrim, Epidiolex, Phenobarbital, Gabapentin, Baclofen, and even a Clonodine patch to try and lessen her seizures and neurostorming.
Sadly, they were doing little to help but were very much contributing to her cognitive and motor developmental delays.
What Is Neurostorming in Medical Terms?
Neurostorming is the parent-friendly name for what neurologists and pediatric intensivists call Paroxysmal Sympathetic Hyperactivity (PSH). The condition was first formally defined by an international consensus group in 2014, and a pediatric clinical practice guideline was published in 2023 to help hospitals manage it more consistently in kids.
In plain English, here’s what’s happening:
The brain has been injured. That injury, whether from a car accident, a fall, oxygen deprivation at birth, or a near-drowning, disrupts the brain’s ability to regulate the body’s stress response. The Sympathetic Nervous System, which is supposed to fire up briefly during real danger and then back off, gets stuck in the “on” position. There’s no real threat. But the body acts like there is one, over and over again. At PX Docs, we recognize that this is dysautonomia.
Researchers call this the “disconnection theory“—the cortex (the thinking, regulating part of the brain) loses its connection to the lower brainstem and hypothalamus, resulting in unopposed sympathetic outflow with nothing to put the brakes on it.
These episodes can happen many times a day. They can be triggered by something as small as a position change, a loud noise, or being touched. And every storm wears the child’s body and brain down a little more.
What Are the Symptoms of Neurostorming?
Symptoms of Neurostorming include rapid heart rate, high fever, elevated blood pressure, rapid breathing, heavy sweating, rigid posturing, and increased muscle tone—all occurring together in episodes that can last minutes to hours. The current consensus diagnostic criteria for Paroxysmal Sympathetic Hyperactivity require simultaneous, paroxysmal episodes including most of the following:
- Tachycardia (rapid heart rate)
- Hyperthermia (high fever, often without infection)
- Hypertension (elevated blood pressure)
- Tachypnea (rapid breathing)
- Diaphoresis (heavy sweating)
- Dystonic posturing (muscular contraction, rigid limbs, arched back, tension throughout the body)
- Increased muscle tone
These signs often appear across multiple body systems at the same time, because neurostorming is fundamentally a problem of the Autonomic Nervous System—the master control system that coordinates heart rate, breathing, temperature, digestion, and muscle tone all at once. When the ANS goes haywire, everything it controls does too.
For parents, the storm itself is usually unmistakable. The child becomes rigid, hot, sweaty, and visibly distressed. The episode can last minutes to hours. Afterward, the child is often exhausted.
What Causes Neurostorming in Children?
Neurostorming is most often a downstream consequence of a brain injury. The brain trauma comes first. The dysregulated nervous system response follows.
The most common causes in children include:
- Traumatic brain injury (TBI). Falls, motor vehicle accidents, sports injuries, and abusive head trauma. Pediatric studies report PSH rates ranging from about 13% in children with severe TBI (Pozzi et al., 2017).
- Hypoxic-ischemic encephalopathy (HIE). When a baby’s brain is deprived of oxygen, most commonly during a complicated labor and delivery, the resulting injury can produce neurostorming-like patterns later in development.
- Birth trauma. This is where the conventional medical conversation tends to stop, but it’s where the PX Docs conversation often starts. The use of forceps, vacuum extraction, prolonged labor, cord accidents, and even “routine” pulling and twisting on a baby’s head and neck during delivery can damage delicate brainstem and upper cervical structures. That damage can disrupt the same autonomic pathways involved in PSH.
- Stroke, infection, and tumors. Less common, but documented causes of dysautonomia in pediatric brain injury.
The deeper question is why some children develop full-blown Neurostorming after a brain injury, and others don’t. The honest answer from the research community is that we don’t yet fully know. But the dominant theory—the disconnection theory—points to something every Neurologically-Focused Chiropractor recognizes immediately: when the brain loses its ability to inhibit the sympathetic system, the body has no brake pedal.
How Does Neurostorming Connect to the Nervous System?
Neurostorming is fundamentally a problem of the Autonomic Nervous System—specifically, an imbalance between the sympathetic “fight or flight” branch, which gets stuck in overdrive, and the parasympathetic “rest, digest, and regulate” branch, which fails to bring the body back to baseline. To understand it, you have to understand the two halves of the Autonomic Nervous System and how they’re supposed to work together.
Picture a car. Your child’s nervous system is the driver.
The Sympathetic Nervous System is the gas pedal. It fires up when there’s danger, exercise, or stress. Heart rate climbs. Breathing speeds up. Blood pressure rises. Muscles tense. This is “fight or flight” — and in short bursts, it’s lifesaving.
The Parasympathetic Nervous System is the brake pedal. It’s the body’s “rest, digest, and regulate” mode. It slows the heart rate, calms breathing, supports digestion and sleep, and helps the body return to balance after a stress response. The parasympathetic system is run primarily by the vagus nerve, the longest cranial nerve in the body.
In a healthy nervous system, these two systems trade off smoothly. Stress arrives, the gas pedal fires, the threat passes, the brake pedal engages, and the body returns to baseline.
In neurostorming, the gas pedal is stuck to the floor—and the brake pedal isn’t working. That state of imbalance has a name: dysautonomia. Dysautonomia is an imbalance within the Autonomic Nervous System, specifically an overactivation of the sympathetic “fight or flight” response combined with an underactivation of the parasympathetic “rest, digest, and regulate” response, driven primarily by the vagus nerve.
Sympathetic dominance is the engine. Vagus nerve dysfunction is the missing brake. Together, they create the conditions in which Neurostorming becomes possible and where it’s hardest to stop.
Why Is the Vagus Nerve So Important in Neurostorming?
The vagus nerve is the primary driver of the Parasympathetic Nervous System, and when it’s impaired by brainstem injury, birth trauma, or upper cervical subluxation, the body loses its ability to calm down a sympathetic storm. The vagus nerve isn’t just a small player here. It’s the entire parasympathetic regulatory system in one nerve.
The vagus nerve branches off the brainstem at the base of the skull, travels down through the upper cervical spine, and then sends fibers to the heart, lungs, gut, and most internal organs. It’s responsible for slowing heart rate, lowering blood pressure, regulating breathing rhythm, calming the digestive system, and modulating inflammation.
When the vagus nerve is functioning well, it acts as a powerful counterweight to the sympathetic system. The brake pedal is responsive. The body can regulate itself.
When the vagus nerve is impaired—through brainstem injury, birth trauma, upper cervical subluxation, or chronic stress—the brake pedal stops working. The threshold for sympathetic activation drops. Storms become easier to trigger and harder to calm.
This is why so much of our clinical attention is focused on the upper cervical spine and brainstem region. It’s also why vagus nerve dysfunction shows up so consistently in kids with Neurostorming, dysautonomia, and a long list of related challenges.
What Is the “Perfect Storm” Behind Pediatric Neurostorming?
The “Perfect Storm” is a concept developed by Dr. Tony Ebel describing the cumulative sequence of neurological stressors—prenatal stress, birth trauma, and early childhood toxic load—that can overwhelm a child’s developing nervous system, leading to subluxation, dysautonomia, and chronic health challenges. Most parents we see haven’t had a single catastrophic event. They’ve had a sequence, and that sequence is what we call the “Perfect Storm.”
Here’s how it shows up in kids who go on to experience neurostorming:
- Prenatal stress and pregnancy challenges. Maternal stress, anxiety, medications, and difficult pregnancies bathe the developing fetal nervous system in stress hormones. The baby’s Autonomic Nervous System is already shifting toward sympathetic dominance before birth.
- Birth trauma and interventions. C-sections, forceps, vacuum extraction, prolonged labor, induction, and cord accidents apply mechanical and physiological stress to the brainstem, upper cervical spine, and vagus nerve at the most fragile moment in the child’s life. This is where many of the brain injuries underlying neurostorming are seeded.
- Early childhood stressors. Repeated illnesses, antibiotic exposure, environmental toxins, and unaddressed neurological dysfunction stack on top of the existing imbalance. The nervous system never gets a chance to recover and regulate.
For Scarlett, the “Perfect Storm” wasn’t theoretical. It was her actual story, a stressful pregnancy, a rough labor and delivery, then seizures and storms by her first birthday. By the time her family found us, the medical system had given her six different medications to suppress symptoms and zero interventions to address the underlying dysregulation.
This is the gap that Neurologically-Focused Chiropractic Care was built to fill.
How Does Subluxation Contribute to Neurostorming?
Subluxation is a pattern of neurological dysfunction in the spine characterized by three components:
- Misalignment within the neurospinal system
- Fixation or restricted joint motion
- Neurological interference that disrupts communication between the brain and body.
When physical trauma, especially birth trauma or head injury, affects the upper neck and brainstem region, it often produces this pattern.
All three components matter. It’s not just a “bone out of place.” It’s a functional problem in which the joint stops moving properly, the brain stops getting clear sensory input from that joint, and the entire neurological feedback loop becomes distorted.
When subluxation shows up in the upper cervical or upper thoracic region, the same region where the vagus nerve exits the brainstem, it tends to interfere with parasympathetic function. The brake pedal weakens. Sympathetic dominance grows. And the threshold for nervous system dysregulation drops.
That’s why kids with chronic neurostorming so often present with the same patterns we see in dysautonomia, Sympathetic Nervous System overdrive, and severe vagal dysfunction. The label changes. The underlying mechanism doesn’t.
How Does Neurologically-Focused Chiropractic Care Address Neurostorming?
Neurologically-Focused Chiropractic Care addresses Neurostorming by identifying and reducing subluxation patterns in the upper cervical and brainstem region, restoring vagus nerve function, and helping the Autonomic Nervous System shift out of chronic sympathetic dominance toward better regulation. It’s important to note that this technology does not diagnose medical conditions, and Neurologically-Focused Chiropractic Care is certainly not a treatment or cure for neurostorming or any other condition, not even back pain. Instead, INSiGHT Scans help us track down the root cause of nervous system dysfunction and dysregulation, and build customized care plans and adjusting protocols to help shift the nervous system back into a state of balance, regulation, and resilience.
INSiGHT Scans are a set of three neurological assessment technologies used by Neurologically-Focused Chiropractors:
- Heart Rate Variability (HRV) testing
- Surface EMG (sEMG)
- Infrared thermography.
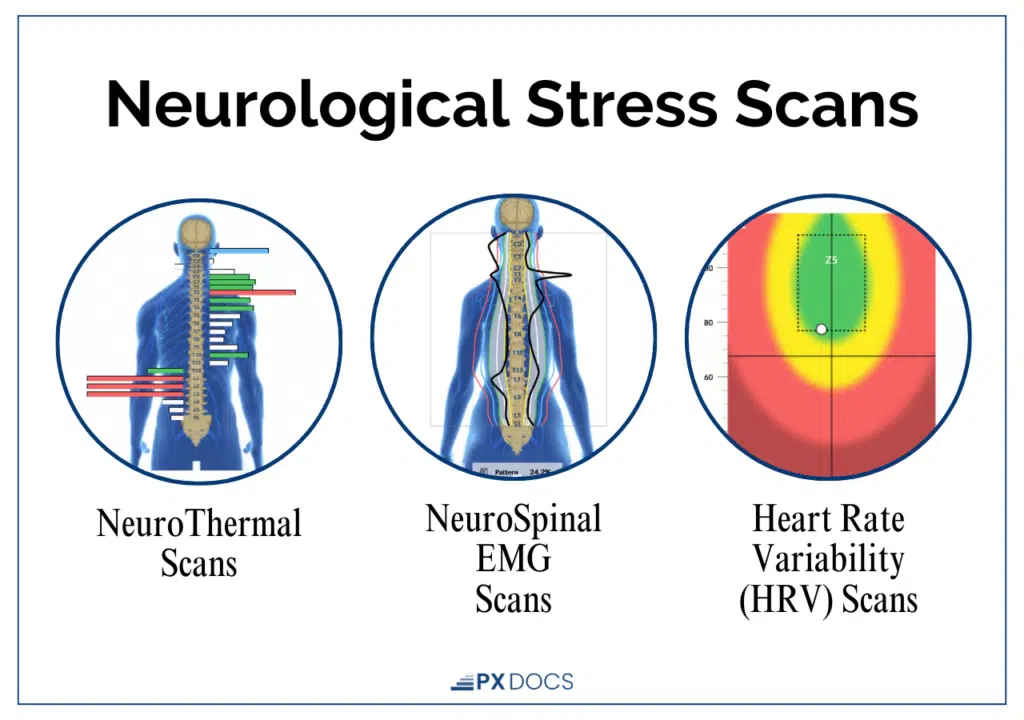
Together, they objectively measure nervous system function, subluxation patterns, and autonomic balance, giving us a clear picture of vagal tone and sympathetic-parasympathetic regulation in real time.
How Does Neurostorming Connect to Other Pediatric Conditions?
Neurostorming sits inside a much larger family of conditions, all driven by the same underlying mechanism: a dysregulated Autonomic Nervous System stuck in sympathetic dominance with poor vagal tone.
Children we see with neurostorming often share neurological patterns with kids carrying diagnoses of Autism, ADHD, Sensory Processing Disorder, severe sleep dysregulation, and emotional dysregulation. The labels are different. The neurology is strikingly similar.
That’s why the “Perfect Storm” framework matters so much. The same prenatal stress, birth trauma, and early childhood stressors that produce dysautonomia and neurostorming in one child can produce sensory challenges, attention difficulties, or autism-spectrum patterns in another. The root mechanism is shared.
This is also why kids who get neurological care that addresses the root often see improvements that ripple far beyond the specific condition that brought them in.
What’s the Long-Term Outlook for a Child With Neurostorming?
Outcomes vary enormously. They depend on the severity of the underlying brain injury, how early the child receives care, how well the storming is managed, and whether anything is done to address the underlying nervous system dysregulation rather than just suppressing the storms.
What we see in our offices is that families who add Neurologically-Focused Chiropractic Care to their child’s broader care team often report meaningful gains: fewer, less intense storms, better sleep, improved digestion, greater motor development, and a calmer, more regulated child.
We’re not curing brain injuries. We’re helping children’s nervous systems function better with the brains they have. And for many of these families, that difference is everything.
Finding Help for Your Child
Neurostorming is a severe, often distressing condition that arises in the wake of traumatic brain injuries, particularly in children. Early and accurate identification of symptoms, combined with comprehensive care strategies, can greatly improve outcomes for affected individuals. The role of specialized pediatric care, such as that provided by PX Docs, is indispensable in caring for this challenging condition.
For Scarlett, within the first week of her Neuro Intensive Adjusting Program that we offer through our practice, she started to experience less neurostorming, as well as improvements in sleep, digestion, and motor function. This led to a major improvement in her quality of life, and she has continued to see incredible improvement with ongoing care back home with her PX Doctor in California.
If you suspect your child is experiencing neurostorming, or if you are seeking expert advice on drug-free care that addresses the root cause of the condition, we encourage you to reach out and find a PX Doc specializing in Neurologically-Focused Pediatric Chiropractic Care to ensure the best possible outcome for your child.
Frequently Asked Questions About Neurostorming
What’s the difference between Neurostorming and a seizure? Neurostorming and seizures can look similar from the outside, but they’re different conditions. Seizures involve abnormal electrical activity in the brain and typically show up on an EEG. Neurostorming is autonomic dysregulation, a runaway Sympathetic Nervous System response without the EEG signature of a seizure. Many children, like Scarlett, have both.
Can Neurostorming go away on its own? For some children with milder brain injuries, storming episodes do decrease as the brain heals over weeks or months. For children with more severe injuries or persistent autonomic dysregulation, the pattern often becomes chronic without targeted intervention to address the underlying nervous system dysfunction. Early identification and a coordinated care plan that includes both medical management and nervous system support consistently produce better outcomes.
Is Neurostorming the same as Paroxysmal Sympathetic Hyperactivity (PSH)? Yes. “Neurostorming” is the parent- and clinician-friendly term that’s spread through ICU and rehabilitation communities, while “Paroxysmal Sympathetic Hyperactivity” is the formal medical term used in research papers and pediatric clinical practice guidelines. They describe the same condition, episodes of extreme autonomic dysregulation following brain injury, and can be used interchangeably in conversations between families and medical providers.
Is chiropractic care safe for a child who has neurostorming? Neurologically-Focused Chiropractic Care for medically complex children uses gentle, low-force, neuro-tonal adjustments—not the high-velocity manipulations many adults associate with chiropractic. PX Docs are specifically trained to work with children who have brain injuries, seizure conditions, and significant medical complexity, often in coordination with the child’s medical team.
Can chiropractic care replace my child’s neurostorming medications? No. Decisions about medication changes always belong to your child’s medical team. What Neurologically-Focused Chiropractic Care offers is a complementary approach that addresses underlying nervous system regulation. Many families find that as their child’s nervous system regulates better, conversations about medication adjustments become possible, but those conversations always happen with the prescribing physician.
What’s the connection between birth trauma and Neurostorming? Birth trauma—including forceps, vacuum extraction, prolonged labor, cord accidents, and hypoxic events—can damage the brainstem, upper cervical spine, and vagus nerve. These are the exact structures involved in autonomic regulation. Children with significant birth trauma are at higher risk for the kind of neurological dysfunction that underlies neurostorming, dysautonomia, and a range of related challenges. How do I find a chiropractor who works with Neurostorming? Look for a Neurologically-Focused Chiropractor who specializes in pediatric care, uses INSiGHT Scans for objective neurological assessment, and has experience working with medically complex children. The PX Docs Directory lists practitioners trained in this specific approach, including doctors who routinely work with families navigating brain injury, seizure conditions, and severe autonomic dysregulation.



